George Martin, MD
Dermatology and Laser Center of Maui, Kihei, Hawaii
Disclosure: Dr. Martin is a medical consultant for DUSA Pharmaceuticals, Inc., and has served on the scientific advisory boards for DUSA Pharmaceuticals, Inc., Galderma, Sanofi-Aventis, Abbott Laboratories, LEO Pharma, and Medicis Pharmaceutical Corporation. He is also a speaker for DUSA Pharmaceuticals, Inc., Medicis Pharmaceutical Corporation, and Graceway Pharmaceuticals. He does not own stock in any of these companies. Editorial support for this article, funded by Dermik Laboratories, a business unit of Sanofi-Aventis U.S. LLC, was provided by Al Balkiewicz, MSc, and Santo D’Angelo, PhD, of Peloton Advantage, LLC. The author was fully responsible for the content, editorial decisions, and opinions expressed in the current article and did not receive an honorarium related to the development of this manuscript.
Abstract
Actinic keratosis is one of the most common diagnoses made by dermatologists. Many experts recommend treating all actinic keratoses because of their potential to progress to invasive squamous cell carcinoma. Physicians have a large armamentarium of actinic keratosis treatment modalities available to them, including destructive therapies, such as cryotherapy, curettage and electrodessication, chemical peels, photodynamic therapy, and topical therapies, including 5-fluorouracil, imiquimod, and diclofenac. In addition to standardized monotherapy regimens, combinations of two concomitant or sequential therapies and alternative topical dosing regimens have been studied in a number of clinical trials. Such therapeutic courses are used to maintain or enhance efficacy while improving tolerability, convenience, and/or patient adherence. This abundance of treatment options prompted development of several actinic keratosis management guidelines. Whereas two sets of treatment guidelines were published by European organizations within the past three years, the most recent United States-based guidelines for dermatologists were published by the American Academy of Dermatology in 1995. Because they are not up to date, the 1995 United States guidelines lack recent clinical developments and an evidence rating system and can no longer effectively guide practitioners. While there are benefits and potential limitations to developing an updated set of United States-based guidelines, there is a clearly defined need for a unified, comprehensive, evidence-based guideline approach to actinic keratosis treatment that balances the need to tailor long-term management of the disease to the needs of the individual patient.
(J Clin Aesthet Dermatol. 2010;3(11):20–25.)
Actinic keratosis (AK) is the second most common diagnosis made by dermatologists.[1] From 2000 to 2003, an estimated 5.2 million United States physician visits for AK occurred annually, incurring approximately $920 million in direct costs for the physician and treatment. Since that time, the incidence of AK and the associated number of physician visits appear to be rising.[2,3]
The worldwide incidence of AK is difficult to estimate, given that prevalence varies depending on the population evaluated.[4] Risk factors for developing AK include fair skin type, immunosuppression, and cumulative ultraviolet (UV) exposure.[5–7] AKs are more common in men, persons with occupational exposure to the sun, and those living closer to the equator.[5–8] The risk of developing AKs is also directly associated with age.[4] In northwest England, one evaluation showed that the prevalence of AK was 34.1 percent for men older than 70 years, but only 3.6 percent for those aged 40 to 49 years.[9]
AK is thought to be part of a biological continuum of cellular and clinical abnormalities that begin with photodamaged skin and can culminate in the formation of invasive SCC.[7,10] Although the risk of progression of AK to nonmelanoma carcinoma is not clearly defined, it has been suggested that AK progresses to squamous cell carcinoma (SCC) in approximately 10 percent of cases within about two years.[6,11,12] New evidence suggests that lesions clinically diagnosed as AK can also progress to basal cell carcinoma (BCC).[13] In a recent longitudinal study of high-risk men, the four-year risk of AK developing into SCC was 2.57 percent and into BCC was 1.56 percent.[13] However, histological examination of 459 SCC cases has demonstrated that more than 97 percent of SCC lesions arise from or form in close proximity to AKs.[14]
Although SCC is not typically associated with high mortality rates,[15] perineural involvement and deep or large SCC lesions increase morbidity and mortality.[16] Up to 65 percent of AKs may clinically regress over five years,[13] but, because it is impossible to know which lesions will progress to invasive SCC, it is recommended that all AKs be treated.[6,8,17–21]
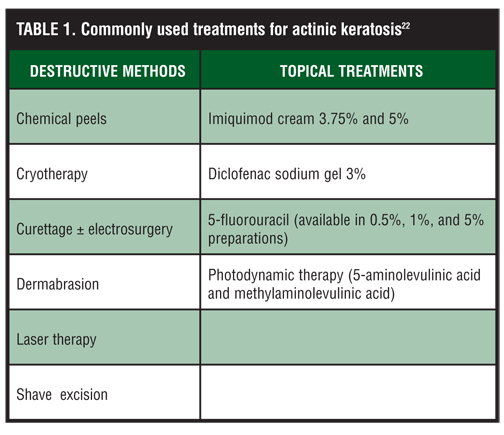
A variety of safe and efficacious treatments are available for AKs that have specific risks and benefits. Some treatments must be administered by the physician while others are applied topically by the patient. Some patients require surgical procedures requiring local or regional anesthesia. Lesion-directed therapies typically use physically destructive modalities to treat individual lesions in a short period (e.g., one office visit). Field-directed therapies use topical agents to treat multiple AKs over a large treatment area; they generally require weeks to months of use, but have the potential to treat subclinical lesions.[22,23] Table 1 lists commonly used AK therapies.
{kind=link}
In addition to the monotherapy treatment protocols that were developed to optimize results for United States Food and Drug Administration (FDA) approval, regimens combining two concomitant or sequential AK treatments were assessed in clinical trials. These trials were generally initiated by the investigator, involved fewer patients, and were less well controlled, but still provide valuable clinical information. These combinations—developed to enhance efficacy of individual therapies while improving tolerability, convenience, and/or patient adherence—include sequential 5-fluorouracil (5-FU; 5% cream) and photodynamic therapy (PDT),[24] sequential PDT and imiquimod,[25] sequential diclofenac and cryotherapy,[26] concomitant 5-FU (5% cream) and imiquimod,[27] concomitant 5-FU cream and tretinoin,[28] and sequential 5-FU (0.5% cream) and cryotherapy.[29] To further improve tolerability (e.g., minimize inflammation), investigators also evaluated alternative dosing regimens, including interval or pulse therapy and cycle therapy.[30,31]
An abundance of AK treatment options, various methods of administration, emerging clinical study data, and a heterogeneous patient population necessitate the use of management guidelines. The most recent US-based guidelines for dermatologists were published in 1995 by the American Academy of Dermatology (AAD),[8] and, as a result, lack both recent clinical and drug developments and a rating system for evidence. In this review, the author examines the need for more current US guidelines in light of more recent European guidelines and the need to balance a unified, comprehensive, evidence-based treatment approach against individualized long-term management.
Current Status of AK Management Guidelines
US-based guidelines. The 1995 AAD guidelines describe the diagnosis and epidemiology of AK in a manner consistent with the then-current understanding of the disease, but without practical information on current treatments to guide clinicians. For example, the guidelines do not address the utility of field-based therapy, but describe destructive therapies in detail. Furthermore, therapies such as imiquimod, diclofenac, and PDT are not addressed. In addition, of the few topical therapies that are mentioned (e.g., 5-FU), no information is given on their mechanism of action, benefits, or adverse effects. The 1995 AAD guidelines also fail to provide comprehensive suggestions for appropriate treatments for individual patients. Instead, guidance is limited to several cursory statements. Finally, these guidelines do not provide information on the level of evidence upon which treatment recommendations are made.
Since the 1995 AAD guidelines were published, several practical reviews of AK treatments have appeared in the literature, including a US-based consensus recommendation directed toward primary care physicians (PCPs). These papers present more recent clinical data, new drug approvals, and trends in clinical practice. For instance, Berman et al published consensus panel recommendations aimed at family practitioners in 2006,[2] McIntyre et al reviewed AK treatments directed at PCPs in 2007,[32] and a 2004 review by Jorizzo et al[33] and a 2006 review by Gold and Nestor[20] directed their discussions at dermatologists. These papers provide some updated guidance on the selection of therapy for their respective audiences.
Outdated US guidelines: Impact on clinical practice. Whereas the impact of outdated US guidelines for the treatment of AK cannot be easily quantified, one disadvantage is that neither dermatologists nor PCPs have a primary information resource for treating patients with AKs. Without such a resource, these clinicians do not have comparative data readily available for the key contemporary approaches to treatment.
Alternative concentrations of topical medications, dose adjustment–based treatment approaches, interval or pulse therapies or cycle therapy, and combinations of destructive and topical modalities are examples of treatment approaches that have evolved over the past decade in attempt to improve efficacy and tolerability. The use of lower-concentration medications (e.g., 5-FU cream 0.5%, imiquimod 3.75% cream), short-contact PDT (e.g., reduced aminolevulinic acid [ALA] incubation times),[34–36] and reduced treatment durations (e.g., topical 0.5% 5-FU cream for 1 week or 5% imiquimod three times weekly for 1 month on/1 month off/1 month on)[37–39] all improved tolerability and showed comparable efficacy. Interval, pulse, and cycle therapies with 5-FU and imiquimod, for which the duration of treatment exposure is shorter than conventional treatment periods, were also shown to provide comparable efficacy while minimizing irritation and erythema typically associated with topical treatments.[30,31,40,41] For example, combination therapy with 5-FU (5% cream) and short-course ALA-PDT was as effective as standard courses of ALA-PDT alone.[24] In addition, the combination allowed for shorter duration of 5-FU use (resulting in less severe irritation) and more convenient ALA incubation periods (only one office visit required).[24]
Destructive treatments featured prominently in the 1995 guidelines are still a standard of therapy despite the effectiveness of topical therapy for the treatment of widespread lesions. A study examining data from the Medicare Current Beneficiary Survey and National Ambulatory Medical Care Survey showed that 51 percent of the $920 million spent annually on the treatment of AK was spent on destructive treatments compared with six percent spent on topical therapies.[3] Although the apparent less-frequent use of topical therapies may be related to associated tolerability and compliance issues,[42] it also suggests a potential disadvantage of outdated treatment guidelines that do not provide guidance on those newer therapies aimed at improved tolerability and reduced severity of adverse events.
European guidelines. Two European organizations more recently published guidelines for the management and treatment of AK: the European Dermatology Forum[21] in 2006 and the British Association of Dermatologists[43] in 2008. Both guidelines provide recommendations on selecting treatments in accordance with patient characteristics and clinical presentation of AK.[21,43] The British Association of Dermatologists guideline recommendations are based on efficacy, ease of use, and cost-benefit information.[43] These guidelines, while relying on data acquired before 2004, provide information on such recent treatments as PDT, diclofenac gel, imiquimod cream, and alternative 5-FU formulations and dosing regimens.[21,43]
Unlike the older US guidelines, the two European guidelines use a taxonomic system to rate the strength of evidence upon which recommendations were made.[21,43] Moreover, both summarize the current safety and efficacy data for destructive and field-based therapies. The European Skin Academy also recently published a five-step treatment algorithm for AK treatment decisions.[23] The steps detailed in the algorithm are 1) initial diagnosis, 2) decision to treat, 3) treatment approach, 4) treatment selection factors, and 5) treatment choice. While partially evidence based, the algorithm also represents a consensus from key European opinion leaders.
Updated European guidelines: Impact on clinical practice. While the lack of updated guidelines leaves US clinicians without a centralized resource for taxonomic classification of treatment approaches, European dermatologists and PCPs have comprehensive documents outlining later advances in the diagnosis and treatment of AK. Unquestionably, the European guidelines present information and guidance relevant to practitioners in the United States. However, differences between the United States and Europe in available treatments, insurance systems, medication costs, and regulatory approval limit the use of the European guidelines. In addition, clinical concepts surrounding the treatment of AK in the European setting reflect attitudes and practices that are vastly different than those in the US. This, combined with the fact that certain treatments approved in the United States are not available or approved in the United Kingdom (e.g., ALA-PDT 3.75% imiquimod), represents a significant treatment gap that is left unfulfilled with any current AK-based published guidelines.
The most recent European-based guidelines also have an unavoidable consequence that affect all published guidelines—the inability to keep up with the ever-evolving treatments and regimens that are studied and published each year. While the British Academy of Dermatology guidelines were published in 2008, the recommendations provided were primarily based on published evidence from 1966 to 2004.[43] Since 2004, numerous treatment options have been introduced and/or studied extensively, providing evidence from which to base additional or more appropriate treatment recommendations. The use of combination therapies, as well as interval or short-course treatment approaches, has also been included in the treatment armamentarium since that time, adding another layer of management options for AK. Most importantly, the understanding of AK pathophysiology, particularly in terms of its close relationship and parallels to SCC in situ, has grown substantially in the past five years, further heightening the importance of treating AKs at all levels of its severity/progression.
Evaluating the Need for New US Guidelines for AK
Need for updated guidelines. The therapies discussed in the 1995 AAD guidelines no longer provide adequate guidance for managing AKs. For example, masoprocol is no longer available in the United States, and diclofenac, new formulations of imiquimod and 5-FU, and PDT using 5-ALA and methylaminolevulinic acid (MAL) were all approved for the treatment of AK within the past 15 years.[44–46] In addition, while intralesional interferon and systemic retinoids are no longer considered routine treatments for AK, evidence now supports the safety and efficacy of PDT.[20]
A wealth of data on the efficacy of existing treatments has also emerged since 1995. For example, the first prospective study evaluating the efficacy of cryotherapy was conducted in 2004 despite its being a mainstay of AK therapy in 1995.[47] In this study, the 67.2-percent observed cure rate was substantially lower than the observed cure rates of 98 percent previously reported[48] and the long-term outcomes of field-based therapies that are still under investigation.[49–52] Also, in the past 10 years, studies have investigated new dosing regimens for topical therapies and regimens combining multiple treatment modalities.[24–27,29–31] The data from these studies were unavailable in 1995 and should be incorporated into new guidelines.
Although considerable advances in AK research were made and studies of individual treatments were conducted in the past 15 years, few head-to-head, controlled studies of AK treatments were performed and, of these, most compared two topical therapies.[53–55] In 2007, Krawtchenko et al were the first to compare three common treatments for AK (i.e., 5-FU, imiquimod, and cryotherapy).[41] The paucity of comparative studies makes it difficult for physicians to effectively practice evidence-based medicine when selecting from among available AK treatment regimens.[32] Given the lack of comparative data, a need exists to gather and rate the strength of available evidence to aid decision making and establish a consistent approach to AK treatment among US physicians.
Refuting the need for updated US guidelines. There are some potential arguments against developing updated US-based AK management guidelines. For example, the numerous variations in presentation of AKs (e.g., number, type, location of lesions) and patient characteristics (e.g., medical status, tolerance for inflammation), in conjunction with the variety of available treatments, suggest that uniform guidelines will not be practical. Also, while there are numerous differences that limit the overall applicability of recent European guidelines to an American audience, the counter-argument could be made that the meta-analysis and evidence grading of recent clinical data make the European guidelines useful enough to US-based physicians despite the differences between the two healthcare systems. For that matter, healthcare differences within the United States and the variety of practitioners managing AK (e.g., internal medicine and PCPs, dermatologists) could make a single US-based set of management guidelines too idealistic if not too labor- and time-intensive to create.[1]
AKs have the potential to progress to skin carcinoma or to clinically regress spontaneously.[6,11,13] Although some physicians consider all AKs as early SCC,[18] this belief is not universally accepted. The lack of a consensus regarding the classification of AKs precludes a globally accepted theory for AK/SCC pathogenesis and treatment. In fact, the guidelines prepared by the British Association of Dermatologists propose that “no therapy or emollient is a reasonable option for mild AKs.”[43] Although predicting the course of individual AKs is impossible, evidence suggests that lesions that are indurated or inflamed, larger than 1cm, rapidly enlarging, bleeding, erythematous, or ulcerated are more likely to progress to SCC.[56]
Physicians must recognize that current treatments must be individualized to the patient. Each treatment has benefits and risks, making the creation of a single treatment algorithm for all patients implausible. The lack of standardization of physician-administered therapies further complicates the creation of treatment guidelines. For example, the efficacy of cryotherapy is directly associated with the duration of cryogen application, a characteristic that appears to vary greatly among physicians.[47] Accounting for such variation poses a challenge in standardizing treatment guidelines.
Any argument against the development of new US-based guidelines should be tempered by the need of physicians to remain educated about advancements in dermatology and AK management. The need for well-designed, well-controlled, clinical studies evaluating treatments for AKs continues. Fortunately, treatment reviews covering new developments and clinical data help physicians to make informed treatment decisions. Such reviews have the benefit of being tailored to the needs of their target audience.
Future Directions
The management of AKs is complex for physicians, requiring frequent follow up and often necessitating long-term management.[21] Selection of a treatment regimen should be individualized for the patient and should weigh a wide range of factors beyond the safety and efficacy of each (Figure 1).[22] Given the complexities of AK management, many physicians would benefit from a document on treatment selection and ranking of the current evidence. Whether such a document must take the form of a US treatment guideline is debatable, and some may argue that the development and review process for guidelines, often lengthy and intricate, would not result in guidelines appreciably different from recent European guidelines. A worthwhile alternative to new US-based guidelines would be a consensus document combining available evidence with the expert opinion of a small group of key US thought leaders. Such a document would combine evidence already rigorously reviewed by others while being applicable to physicians and patients in the United States and helping physicians identify the optimal treatment approach for their AK patients.
{kind=link}
Ongoing research continues to expand our understanding of the pathogenesis of AK and to highlight the strengths and weaknesses of current treatment options. Given the time constraints of daily clinical practice, physicians are challenged to maintain a current understanding of the overall evidence base. A single, unifying document that rates the current evidence and provides consensus guidelines for treatment would help overburdened clinicians practice evidence-based medicine with the most up-to-date evidence and avoid such treatment issues as increased adverse events or decreased reduction and clearance of AKs. The creation of an updated consensus document would provide a meaningful reference for clinicians that could be used to improve AK treatment, increase the chances for optimal patient outcomes, and even facilitate a more productive open dialog among dermatologists and others treating patients with AKs.
References
1. Fleischer AB Jr, Herbert CR, Feldman SR, O’Brien F. Diagnosis of skin disease by nondermatologists. Am J Manag Care. 2000;6:1149–1156.
2. Berman B, Bienstock L, Kuritzky L, et al. Actinic keratoses: sequelae and treatments. Recommendations from a consensus panel. J Fam Pract. 2006;55(Suppl):1–8.
3. Warino L, Tusa M, Camacho F, et al. Frequency and cost of actinic keratosis treatment. Dermatol Surg. 2006;32: 1045–1049.
4. Frost CA, Green AC. Epidemiology of solar keratoses. Br J Dermatol. 1994;131:455–464.
5. Salasche SJ. Epidemiology of actinic keratoses and squamous cell carcinoma. J Am Acad Dermatol. 2000;42(1 Pt 2):S4–S7.
6. Rossi R, Mori M, Lotti T. Actinic keratosis. Int J Dermatol. 2007;46:895–904.
7. Schwartz RA, Bridges TM, Butani AK, Ehrlich A. Actinic keratosis: an occupational and environmental disorder. J Eur Acad Dermatol Venereol. 2008;22:606–615.
8. Drake LA, Ceilley RI, Cornelison RL, et al. Guidelines of care for actinic keratoses. Committee on guidelines of care. J Am Acad Dermatol. 1995;32:95–98.
9. Memon AA, Tomenson JA, Bothwell J, Friedmann PS. Prevalence of solar damage and actinic keratosis in a Merseyside population. Br J Dermatol. 2000;142:1154–1159.
10. Yantsos VA, Conrad N, Zabawski E, Cockerell CJ. Incipient intraepidermal cutaneous squamous cell carcinoma: a proposal for reclassifying and grading solar (actinic) keratoses. Semin Cutan Med Surg. 1999;18:3–14.
11. Glogau RG. The risk of progression to invasive disease. J Am Acad Dermatol. 2000;42(1 pt 2):S23–S24.
12. Fuchs A, Marmur E. The kinetics of skin cancer: progression of actinic keratosis to squamous cell carcinoma. Dermatol Surg. 2007;33:1099–1101.
13. Criscione VD, Weinstock MA, Naylor MF, et al. Actinic keratoses: natural history and risk of malignant transformation in the Veterans Affairs Topical Tretinoin Chemoprevention Trial. Cancer. 2009;115:2523–2530.
14. Hurwitz RM, Monger LE. Solar keratosis: an evolving squamous cell carcinoma. Benign or malignant? Dermatol Surg. 1995;21:184.
15. Gloster HM Jr, Brodland DG. The epidemiology of skin cancer. Dermatol Surg. 1996;22:217–226.
16. Clayman GL, Lee JJ, Holsinger FC, et al. Mortality risk from squamous cell skin cancer. J Clin Oncol. 2005;23:759–765.
17. Patients urged to seek treatment for actinic keratoses, recommends the American Academy of Dermatology, the American Cancer Society, and the Skin Cancer Foundation. Cutis. 1999;63:348.
18. Lober BA, Lober CW. Actinic keratosis is squamous cell carcinoma. South Med J. 2000;93:650–655.
19. Mittelbronn MA, Mullins DL, Ramos-Caro FA, Flowers FP. Frequency of pre-existing actinic keratosis in cutaneous squamous cell carcinoma. Int J Dermatol. 1998;37:677–681.
20. Gold MH, Nestor MS. Current treatments of actinic keratosis. J Drugs Dermatol. 2006;5(2 Suppl):17–25.
21. Stockfleth E, Kerl H. Guidelines for the management of actinic keratoses. Eur J Dermatol. 2006;16:599–606.
22. Jorizzo JL, Carney PS, Ko WT, et al. Matching patients with therapy. Cutis. 2004;74(6 Suppl):5–8.
23. Stockfleth E, Ferrandiz C, Grob JJ, et al. Development of a treatment algorithm for actinic keratoses: a European consensus. Eur J Dermatol. 2008;18:651–659.
24. Gilbert DJ. Treatment of actinic keratoses with sequential combination of 5-fluorouracil and photodynamic therapy. J Drugs Dermatol. 2005;4:161–163.
25. Shaffelburg M. Treatment of actinic keratoses with sequential use of photodynamic therapy; and imiquimod 5% cream. J Drugs Dermatol. 2009;8:35–39.
26. Mastrolonardo M. Topical diclofenac 3% gel plus cryotherapy for treatment of multiple and recurrent actinic keratoses. Clin Exp Dermatol. 2009;34:33–35.
27. Price NM. The treatment of actinic keratoses with a combination of 5-fluorouracil and imiquimod creams. J Drugs Dermatol. 2007;6:778–781.
28. Bercovitch L. Topical chemotherapy of actinic keratoses of the upper extremity with tretinoin and 5-fluorouracil: a double-blind controlled study. Br J Dermatol. 1987;116: 549–552.
29. Jorizzo J, Weiss J, Vamvakias G. One-week treatment with 0.5% fluorouracil cream prior to cryosurgery in patients with actinic keratoses: a double-blind, vehicle-controlled, long-term study. J Drugs Dermatol. 2006;5:133–139.
30. Robins P. Pulse therapy with 5-FU in eradicating actinic keratoses with less than recommended dosage. J Drugs Dermatol. 2002;1:25–30.
31. Salasche SJ, Levine N, Morrison L. Cycle therapy of actinic keratoses of the face and scalp with 5% topical imiquimod cream: an open-label trial. J Am Acad Dermatol. 2002;47: 571–577.
32. McIntyre WJ, Downs MR, Bedwell SA. Treatment options for actinic keratoses. Am Fam Physician. 2007;76:667–671.
33. Jorizzo JL, Carney PS, Ko WT, et al. Treatment options in the management of actinic keratosis. Cutis. 2004;74(6 Suppl): 9–17.
34. Smith S, Piacquadio D, Morhenn V, et al. Short incubation PDT versus 5-FU in treating actinic keratoses. J Drugs Dermatol. 2003;2:629–635.
35. Touma D, Yaar M, Whitehead S, et al. A trial of short incubation, broad-area photodynamic therapy for facial actinic keratoses and diffuse photodamage. Arch Dermatol. 2004;140:33–40.
36. Redbord KP, Hanke CW. Topical photodynamic therapy for dermatologic disorders: results and complications. J Drugs Dermatol. 2007;6:1197–1202.
37. Jorizzo J, Stewart D, Bucko A, et al. Randomized trial evaluating a new 0.5% fluorouracil formulation demonstrates efficacy after 1-, 2-, or 4-week treatment in patients with actinic keratosis. Cutis. 2002;70:335–339.
38. Weiss J, Menter A, Hevia O, et al. Effective treatment of actinic keratosis with 0.5% fluorouracil cream for 1, 2, or 4 weeks. Cutis. 2002;70(2 Suppl):22–29.
39. Zeichner JA, Stern DW, Uliasz A, et al. Placebo-controlled, double-blind, randomized pilot study of imiquimod 5% cream applied once per week for 6 months for the treatment of actinic keratoses. J Am Acad Dermatol. 2009;60:59–62.
40. Pearlman DL. Weekly pulse dosing: effective and comfortable topical 5-fluorouracil treatment of multiple facial actinic keratoses. J Am Acad Dermatol. 1991;25:665–667.
41. Krawtchenko N, Roewert-Huber J, Ulrich M, et al. A randomised study of topical 5% imiquimod vs. topical 5-fluorouracil vs. cryosurgery in immunocompetent patients with actinic keratoses: a comparison of clinical and histological outcomes including 1-year follow-up. Br J Dermatol. 2007;157(Suppl 2):34–40.
42. Neidecker MV, Davis-Ajami ML, Balkrishnan R, Feldman SR. Pharmacoeconomic considerations in treating actinic keratosis. Pharmacoeconomics. 2009;27:451–464.
43. de Berker D, McGregor JM, Hughes BR, for the British Association of Dermatologists Therapy Guidelines and Audit Subcommittee. Guidelines for the management of actinic keratoses. Br J Dermatol. 2007;156:222–230.
44. Carac [package insert]. Bridgewater, NJ: Dermik Laboratories; August 2009.
45. Solaraze [package insert]. Fairfield, NJ: Doak Dermatologics; 2007.
46. Aldara [package insert]. Bristol, TN: Graceway Pharmaceuticals, LLC; 2007.
47. Thai K-E, Fergin P, Freeman M, et al. A prospective study of the use of cryosurgery for the treatment of actinic keratoses. Int J Dermatol. 2004;43:687–692.
48. Lubritz RR, Smolewski SA. Cryosurgery cure rate of actinic keratoses. J Am Acad Dermatol. 1982;7:631–632.
49. Lee PK, Harwell WB, Loven KH, et al. Long-term clinical outcomes following treatment of actinic keratosis with imiquimod 5% cream. Dermatol Surg. 2005;31:659–664.
50. Nelson C, Rigel D. Long-term follow up of diclofenac sodium 3% in 2.5% hyaluronic acid gel for actinic keratosis: one-year evaluation. J Clin Aesthet Dermatol. 2009;2:20–25.
51. Stough D, Bucko AD, Vamvakias G, Rafal ES. Fluorouracil cream 0.5% for the treatment of actinic keratoses on the face and anterior scalp. J Clin Aesthet Dermatol. 2008;1:16–21.
52. Witheiler DD, Lawrence N, Cox SE, et al. Long-term efficacy and safety of Jessner’s solution and 35% trichloroacetic acid vs 5% fluorouracil in the treatment of widespread facial actinic keratoses. Dermatol Surg. 1997;23:191–196.
53. Smith SR, Morhenn VB, Piacquadio DJ. Bilateral comparison of the efficacy and tolerability of 3% diclofenac sodium gel and 5% 5-fluorouracil cream in the treatment of actinic keratoses of the face and scalp. J Drugs Dermatol. 2006;5: 156–159.
54. Loven K, Stein L, Furst K, Levy S. Evaluation of the efficacy and tolerability of 0.5% fluorouracil cream and 5% fluorouracil cream applied to each side of the face in patients with actinic keratosis. Clin Ther. 2002;24:990–1000.
55. Kose O, Koc E, Erbil AH, et al. Comparison of the efficacy and tolerability of 3% diclofenac sodium gel and 5% imiquimod cream in the treatment of actinic keratosis. J Dermatolog Treat. 2008;19:159–163.
56. Quaedvlieg PJ, Tirsi E, Thissen MR, Krekels GA. Actinic keratosis: how to differentiate the good from the bad ones? Eur J Dermatol. 2006;16:335–339.