John A. Mouzakis, MD is from University of South Florida College of Medicine, Tampa, Florida. Stephanie Liu, MD and George Cohen, MD are from Department of Dermatology and Cutaneous Surgery, University of South Florida College of Medicine, Tampa, Florida
Disclosure: The authors report no relevant conflicts of interest.
Abstract
Objective: Vitiligo is a common depigmenting condition that carries a high psychosocial morbidity. Many of the current topical and light therapies aid in repigmentation but require extensive treatment periods and carry unwanted side effects. The excimer laser is a newer treatment option that can induce repigmentation in an abbreviated time frame without global exposure to radiation. This case series provides further evidence to support the use of excimer laser in treating vitiligo especially of the face. Design: Patients with extensive facial depigmentation were treated with excimer laser twice weekly and calcipotriene daily until they developed significant repigmentation. Setting: Evaluation and treatment was performed at the Veterans Affairs outpatient dermatology clinic in Tampa, Florida. Participants: Three patients with Fitzpatrick skin types IV to VI were selected. These patients had failed a variety of topical treatments including steroids and calcipotriene, but were light naïve prior to beginning the study. Measurements: The primary outcome measure employed was percent repigmentation by visual estimation. The average dose of radiation, number of treatments, and weeks of therapy were also recorded. Results: All three patients experienced greater than 75 percent repigmentation of their facial vitiligo over a treatment course from 10 to 20 weeks. Conclusion: The excimer laser is a viable treatment for vitiligo and may yield results more expeditiously than other commonly utilized therapies. The rapid response may be correlated with skin type, but a more extensive study needs to be undertaken to further evaluate this correlation.
(J Clin Aesthet Dermatol. 2011;4(6):41–44.)
Vitiligo is believed to be an autoimmune disease that results in the destruction of melanocytes leading to depigmentation. The disease affects approximately one percent of the population worldwide. Studies have demonstrated that the disfiguring nature of vitiligo causes high psychosocial morbidity.[1–3] This is especially pronounced in populations with darker skin tone, likely due to the marked contrast.[1,4]
A variety of treatment regimens are currently employed to repigment the skin. However, many of these require a prolonged treatment course and may yield minimal results. Therapies such as topical steroids rarely achieve more than 50- to 75-percent repigmentation and are cumbersome, requiring multiple daily applications. Further, topical steroids may require a year or more to note significant improvement.[5,6] Less than 50 percent of patients achieve greater than 75-percent repigmentation after 10 months of therapy.7 Other topical therapies including tacrolimus and calcipotriene yield similar results to topical steroids.
Patients with extensive depigmentation may prefer treatment with light therapy due to the large surface area affected. Light therapies include oral or topical psoralens plus ultraviolet A radiation (PUVA), narrowband ultra-violet B radiation (NB-UVB), and excimer laser.
PUVA has long been a mainstay of treatment for vitiligo, but over the last decade NB-UVB has been increasing in use due to decreased incidence of phototoxic side effects.[8,9] However, with both therapies, treatment may take many months, a year, or longer to achieve results.[8–10] PUVA achieved a partial response in 60 percent of patients after a mean of 84.2 treatments.[11] Patients treated with NB-UVB experienced a partial response at four weeks, but mean repigmentation was still less than 50 percent by 12 weeks.[12] There is some evidence that light treatments used in combination with topical agents improve outcomes.[13]
The 308nm excimer laser is a newer treatment option that can yield impressive results in an abbreviated timeframe.10 Nicolaidou et al[10] reviewed the use of excimer laser and demonstrated that 15 to 50 percent of patients achieved greater than 75-percent repigmentation. Notably, excimer laser treatment periods were 15 weeks or less in the overwhelming majority of the studies analyzed.[10] Additionally, there has been some evidence that excimer laser treatment causes faster, more complete repigmentation in patients with higher Fitzpatrick skin types.[13,14]
This case series examines three male patients with Fitzpatrick skin types IV to VI and their results after undergoing combination treatment utilizing excimer laser with calcipotriene.
Materials and Methods
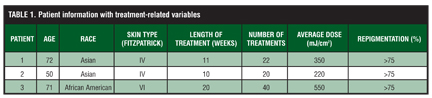
Three male patients presenting with extensive, depigmented, facial macules that were chalk white under Wood’s lamp exam were clinically diagnosed with vitiligo and evaluated in the outpatient dermatology clinic at the Veterans Affairs medical center in Tampa, Florida. These three patients had chronic vitiligo that had been stable for between 3 and 10 years. Two of the patients were Asian with Fitzpatrick type IV skin and one was African American with type VI skin. They had previously undergone therapy with a variety of topical medications including topical steroids and calcipotriene for at least two years (range 2–6 years) without significant repigmentation. The patients were light naïve prior to inclusion in the study. Excimer laser combined with 0.005% calcipotriene topical twice daily was selected for treatment. Laser therapy was performed twice weekly until patients developed significant repigmentation. Patients began using excimer laser at a dose of 200mJ/cm2, which was increased 10 percent per visit until patients experienced phototoxic side effects including marked erythema and blistering. Treatment dosages were then maintained or decreased 10 percent depending on the severity of the side effects. None of the patients stopped treatment due to side effects of the laser therapy. The total number of treatments, the length of time over which the treatments were administered, and the average dose of laser energy exposure were recorded. As in other studies, the authors chose percent repigmentation as their primary outcome measure with ranges of: <25, 25 to 50, 50 to 75, and >75 percent. Figure 1, Figure 2, and Figure 3 show patient pretreatment images. Table 1 contains demographic information and treatment-related variables.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Results
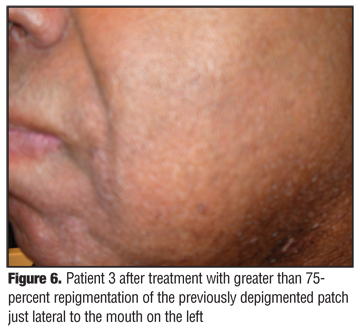
All of the patients completed the recommended treatment course. Figure 4, Figure 5, and Figure 6 illustrate the effect of the combination therapy on the patients. Two of the three patients achieved greater than 75 percent repigmentation after 22 treatments or less. The third patient achieved similar results, but after 40 treatment sessions. There was no correlation between the average dose of laser energy exposure and percent repigmentation.
{kind=link}
{kind=link}
{kind=link}
Discussion
Vitligo is a chronic, psychologically debilitating, and difficult-to-treat condition. Many of the currently utilized therapies demand treatment intervals exceeding one year to achieve demonstrable repigmentation. In this study, patients achieved greater than 75-percent repigmentation of facial lesions between 10 and 20 weeks.
A variety of theories exist to account for the efficacy of light therapy in the treatment of vitiligo. Evidence reveals that inactive melanocytes present in the outer sheaths of hair follicles are spared in individuals with vitiligo. Initiation of therapy then may induce maturation in these latent melanocytes followed by migration upwards along the hair follicle with ultimate dissemination in the epidermis.[15] Perifollicular repigmentation in treated vitiligo and the fact that paucifollicular areas, such as the fingers and genitals, repigment poorly support this theory. Additionally, acral areas characterized by decreased hair-bearing potential are consistently the most refractory regions to therapy.[16,17]
The three patients in this series achieved excellent results (>75% repigmentation) in a short time (5 months or less) in comparison to other treatments, such as topical steroids, PUVA, and NB-UVB. It is the authors’ hypothesis that these patients achieved rapid results with such excellent outcomes because of the increased responsiveness of the facial hair follicles to excimer laser. Future research evaluating the response of the face to excimer laser therapy may provide additional insight into the disease process.
Some research suggests that individuals with higher numerical Fitzpatrick skin type may respond to therapy more quickly and experience better outcomes than their lighter skinned counterparts.[13,14] This study evaluated male, dark-skinned individuals and thus it was not possible for these two factors to be evaluated separately. Further research with larger patient populations stratified by skin type is necessary to more critically evaluate the importance of this variable in achieving repigmentation.
The excimer laser has proven to be a useful tool in the treatment of vitiligo. Patients treated with excimer laser are achieving excellent results in a matter of a few months rather than many months to years. More data is needed to determine whether skin type, sex, or other hair follicle characteristics lend themselves to greater response to excimer therapy. In a broader sense, there is a paucity of data evaluating the relapse rate of patients undergoing any of the light treatments. This information would be crucial to the patient decision-making process and deserves further attention.
References
1. Linthorst Homan MW, Spuls PI, de Korte J, et al. The burden of vitiligo: patient characteristics associated with quality of life. J Am Acad Dermatol. 2009;61(3):411–420.
2. Ongenae K, Beelaert L, van Geel N, Naeyaert JM. Psychosocial effects of vitiligo. J Eur Acad Dermatol Venereol. 2006;20(1): 1–8.
3. Kim do Y, Lee JW, Whang SH, et al. Quality of life for Korean patients with vitiligo: Skindex-29 and its correlation with clinical profiles. J Dermatol. 2009;36(6):317–322.
4. Finlay AY, Ryan TJ. Disability and handicap in dermatology. Int J Dermatol. 1996;35:305–311.
5. Kumaran MS, Kaur I, Kumar B. Effect of topical calcipotriol, betamethasone dipropionate and their combination in the treatment of localized vitiligo. J Eur Acad Dermatol Venereol. 2006;20(3):269–273.
6. Sanclemente G, Garcia JJ, Zuleta JJ, et al. A double-blind, randomized trial of 0.05% betamethasone vs. topical catalase/dismutase superoxide in vitiligo. J Eur Acad Dermatol Venereol. 2008;22(11):1359–1364. Epub 2008 Jun 25.
7. Sanclemente G, Garcia JJ, Zuleta JJ, et al. A double-blind, randomized trial of 0.05% betamethasone vs. topical catalase/dismutase superoxide in vitiligo. J Eur Acad Dermatol Venereol. 2008;22(11):1359–1364.
8. Parsad D, Kanwar AJ, Kumar B. Psoralen-ultraviolet A vs. narrow-band ultraviolet B phototherapy for the treatment of vitiligo. J Eur Acad Dermatol Venereol. 2006;20(2):175–177.
9. Bhatnagar A, Kanwar AJ, Parsad D, De D. Comparison of systemic PUVA and NB-UVB in the treatment of vitiligo: an open prospective study. J Eur Acad Dermatol Venereol. 2007;21(5):638–642.
10. Nicolaidou E, Antoniou C, Stratigos A, Katsambas AD. Narrowband ultraviolet B phototherapy and 308-nm excimer laser in the treatment of vitiligo: a review. J Am Acad Dermatol. 2009;60(3):470–477.
11. Falabella R, Barona MI. Update on skin repigmentation therapies in vitiligo. Pigment Cell Melanoma Res. 2009;22(1):42–65.
12. Klahan S, Asawanonda P. Topical tacrolimus may enhance repigmentation with targeted narrowband ultraviolet B to treat vitiligo: a randomized, controlled study. Clin Exp Dermatol. 2009;34(8):e1029–e1030.
13. Kawalek AZ, Spencer JM, Phelps RG. Combined excimer laser and topical tacrolimus for the treatment of vitiligo: a pilot study. Dermatol Surg. 2004;30(2 Pt 1):130–135.
14. Goldinger SM, Dummer R, Schmid P, et al. Combination of 308-nm xenon chloride excimer laser and topical calcipotriol in vitiligo. J Eur Acad Dermatol Venereol. 2007;21(4): 504–508.
15. Cui J, Shen LY, Wang GC. Role of hair follicles in the repigmentation of vitiligo. J Invest Dermatol. 1991;97(3): 410–416.
16. Anbar TS, Westerhof W, Abdel-Rahman AT, El-Khayyat MA. Evaluation of the effects of NB-UVB in both segmental and non-segmental vitiligo affecting different body sites. Photodermatol Photoimmunol Photomed. 2006;22:157–163.
17. Choi KH, Park JH, Ro YS. Treatment of vitiligo with 308-nm xenon-chloride excimer laser: therapeutic efficacy of different initial doses according to treatment areas. J Dermatol. 2004;31:284–292.