 J Clin Aesthet Dermatol. 2023;16(5):35-39.
J Clin Aesthet Dermatol. 2023;16(5):35-39.
by Mariano Busso, MD and Trevor Born, MD
Dr. Busso is with Dr. Busso Cosmetic Dermatology in Miami, Florida. Dr. Born is with TMB Cosmetic Surgery in Ontario, Canada.
FUNDING: No funding was provided for this article
DISCLOSURES: Drs. Busso and Born are medical advisors to BTL Industries.
ABSTRACT: Background. With many treatments available for managing cellulite, non-invasive procedures are increasingly sought after. Radiofrequency (RF) and targeted pressure energy (TPE) are new techniques developed to counter aesthetic signs of aging. The combination of RF and TPE for cellulite thus requires a more robust investigation.
Objective. We sought to determine the effectiveness and safety of combined/simultaneous RF and TPE for skin tightening and reducing the appearance of cellulite.
Methods. Thirty subjects aged 46.5±9.0 (31–74) years, BMI 19.8-36kg/m2 were enrolled and treated for cellulite on the hips, thighs, abdomen and arms. Each subject received four treatments, over 2 to 4 consecutive weeks. The circumference of the treated areas was measured at baseline, after the final treatment session, and at follow-up visits one month, three months and six months following treatment. The efficacy of the therapy was evaluated based on the Cellulite Severity Scale, Global Aesthetic Index Scale, and the Subject Satisfaction Questionnaire. Occurrence of side effects and adverse events was monitored, therapy comfort was analyzed.
Results. Cellulite severity improved from moderate to mild cellulite (p<0.001) in 95 percent of patients. Blinded, independent, evaluators reported aesthetic improvement in 90 percent of subjects. Significant circumference decrease in the abdomen, hips, and thighs was observed six months after treatment (p<0.01). Eighty-six percent of subjects were satisfied with improved cellulite appearance, and 82 percent of patients reported improved skin laxity. No severe side effects or adverse events occurred.
Conclusion. The simultaneous TPE+RF procedure was able to non-invasively improve cellulite appearance in the majority of subjects and may be recommended for skin tightening on various body parts.
Keywords. Targeted pressure energy, radiofrequency, cellulite, skin laxity, skin rejuvenation, skin tightening, non-invasive, TPE, RF
Cellulite, known as gynoid lipodystrophy or edematous fibrosclerotic panniculopathy is a metabolic disease affecting 80 to 90 percent of post-pubertal females.1–3 The areas affected have large amounts of fat deposition. Cellulite is local, most commonly causing the skin surface topography of the buttocks, posterolateral thighs, and the abdomen, to become dimpled or “orange peel”-like. Problems with peripheral circulation and metabolic failure in normal tissue enhance metabolic failure4 in adipose tissue leading to their degeneration and, progressive fibrosis and sclerosis in the surrounding tissue.5 The focally enlarged fibrous septa form bands, attributable to cellulite, that tether the skin and begin to pull it downwards.6 In relation to the skin surface, perpendicular fibrous septae prevail more in cellulite-presenting women than in men. Thus, cellulite may be a plausible secondary sexual characteristic since males are affected in much fewer instances. The underlying adipose tissue protrudes due to the perpendicular septae in women, whereas the oblique fibers in men seemingly prevent this protrusion.7 Distorted evenness of the dermal-hypodermal interface may also result in physiological changes causing skin surface depressions.8,9
Multiple factors have been posited to influence the occurrence/etiopathogenesis of cellulite including; genetic influence,10 hormonal action (lack of adiponectin in subcutaneous fat, hyperestrogenism),11,12 dermal extracellular matrix changes,13,14 connective tissue architecture, and alterations in microvascular circulation.15 Cellulite management is focused on overcoming the unsightly ripples on the skin surface. Among other techniques,16-18 simultaneous radiofrequency (RF) and targeted pressure energy (TPE) have demonstrated efficacy in improving skin quality and laxity.19-21
The simultaneous emission of monopolar RF (thermal energy) and TPE (mechanical energy) induces collagen remodeling.22 The mechanical stress causes fibrils to dissociate, reducing their thermal stability, hence the temperature required for collagen denaturation is decreased. Controlled thermal heating up to 42°C leads to fibroblast stimulation and neocollagenesis.23 Subcutaneous adipocytes shrink as they undergo apoptosis.19 TPE improves skin elasticity24 and local blood and lymphatic microcirculation,25,26 activates lipolytic enzymes, and increases collagen fiber density.6 Further research is required to document the non-invasive effects and benefits of RF applied synchronously with TPE for treating cellulite.
This study investigated the effectiveness of combined RF and TPE for skin tightening and reducing the appearance of cellulite.
Methods
Thirty subjects (28 female and 2 male) with an average age of 46.5±9.0 (31–74) years and BMI 19.8-36.5kg/m2 were enrolled in this prospective study. The subjects’ Fitzpatrick skin phototypes were: Type II (N=1), Type III (N=14), Type IV (N=12) and Type V (N=3). Subjects aged above 21 years, with pre-treatment cellulite Grade 2 or 3 on the Nürnberger-Muller Scale who were willing to abstain from partaking in any treatments, besides the study procedure, to promote skin tightening and cellulite reduction during the study were included. The subjects needed to maintain regular diet and exercise regimens without extraordinary changes. Exclusion criteria comprised scleroderma, ongoing radiotherapy, pregnancy, cancer, metal or electronic implants, unhealed wounds, ascites, edema, local corticosteroid therapy, deep peeling three months prior, and infection in the treatment area. After subjects obtained concise instructions about the study conduct and provided informed consent, they were enlisted to participate. The study protocol and design were approved by the Advarra Institutional Review Board and adhered to the Helsinki Declaration. This clinical study is registered on clinicaltrials.gov (NCT05624216).
Each subject received four 10- to 25-minute treatments with a device that simultaneously combines RF and TPE (Emtone, BTL Industries) during 2 to 4 consecutive weeks. The treatment area depended on the location where cellulite was present: the hips, thighs, buttocks, stomach, abdomen, and upper arms.
Patient follow-up visits happened one, three, and six months after the final treatment.
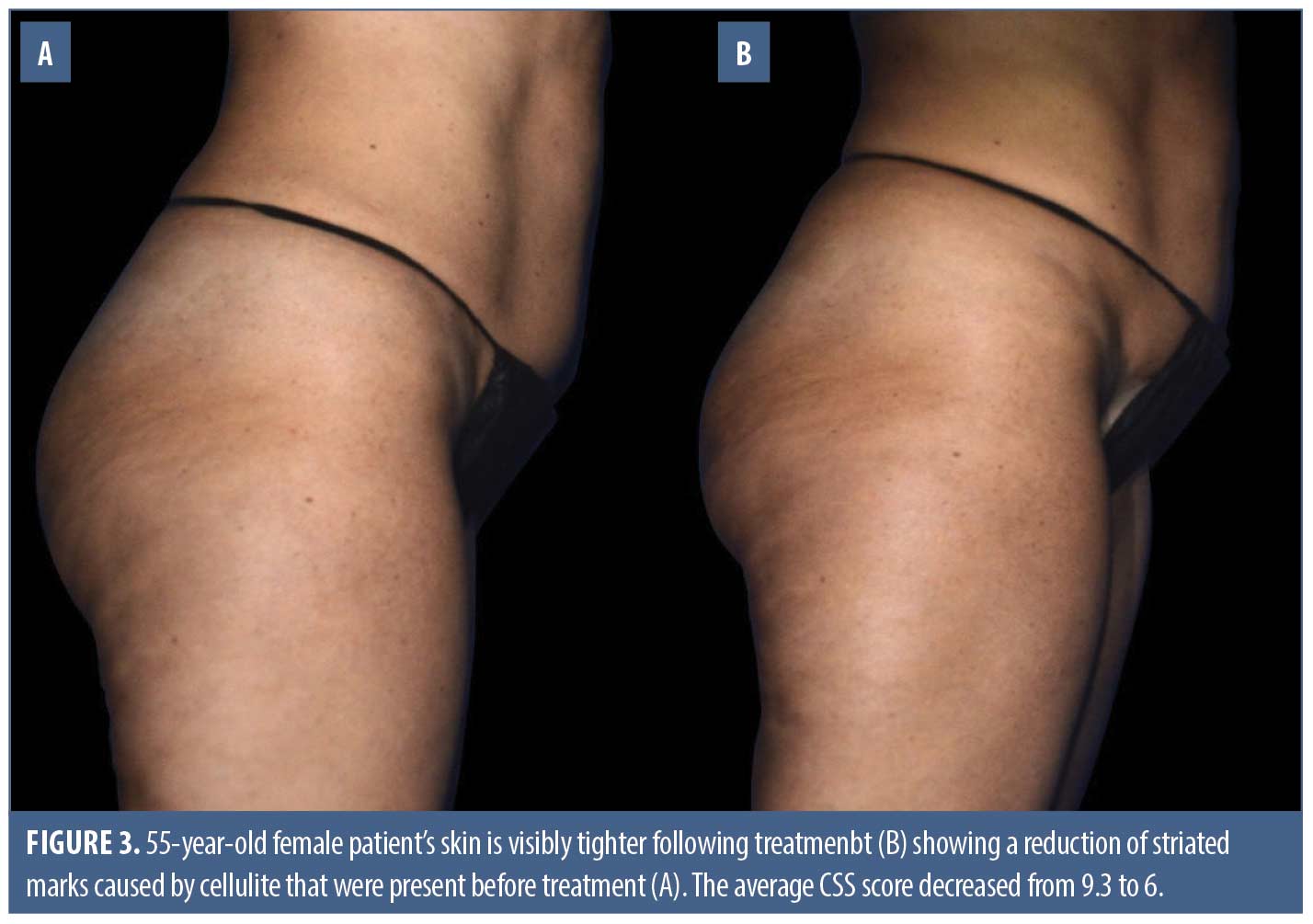
Digital photographs of the treatment area were obtained at baseline and post-treatment follow-up visits.
The efficacy of the treatment was evaluated based on the Cellulite Severity Scale (CSS). Three (blinded/independent) evaluators assessed before and after digital photographs to grade the cellulite extent. The three evaluators used the same pictures to determine improvement in the appearance of the treated area according to the Global Aesthetic Improvement Scale (GAIS).
Circumference of the treated body part was measured at baseline and follow-up visits to determine changes in the subcutaneous adipose layer/tissue thickness. Weight and BMI were also measured at these visits.
Subjects’ satisfaction with treatment results was assessed during the follow-up visits through a 5-point Likert scale questionnaire. Therapy comfortability was evaluated after the final treatment using a 5-point Likert scale and a 10-point numeric rating scale (NRS) assessing the pain level. The occurrence of adverse events and side effects was monitored throughout the study.
Data were statistically analyzed using analysis of variance with Tukey post-hoc test and two-sample t-tests (significance level p=0.05).
Results
Cellulite severity and aesthetic improvement scales. Twenty-eight (n=28) subjects completed the study. Based on photographs obtained pre- and post-treatment, evaluation of the group showed a statistically significant (p<0.001) improvement from moderate cellulite to mild cellulite, decreasing by 4.2 points from 9.1±1.8 at baseline to 4.9±1.9 after six months. Blinded reviewers’ average scores indicated that 95 percent of subjects had improved by the 6-month follow-up visit. The average GAIS score was 1.5±0.6. GAIS Evaluator (Ev) grading on average subjects showed improvement as follows: Ev 1 85 percent, Ev 2 95 percent, and Ev 3 90 percent (average 90% subjects had improved). CSS grading indicated no subjects were left with severe cellulite after the treatments. The majority of subjects had mild cellulite post treatment compared to moderate at baseline (Table 1).

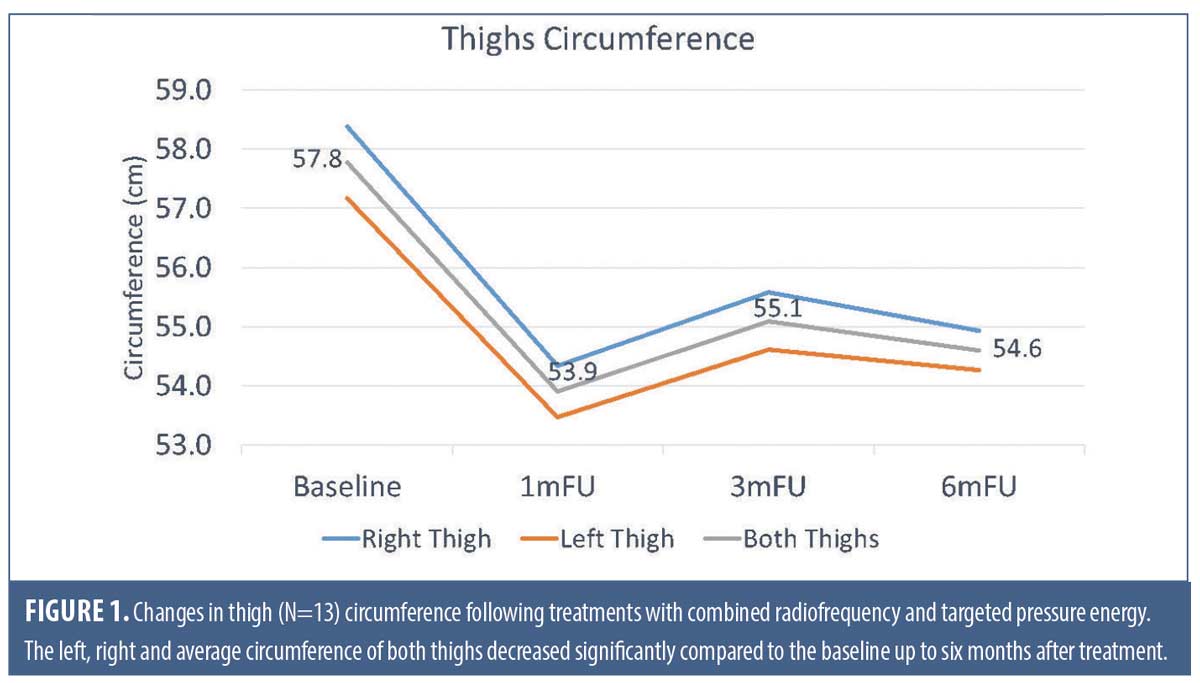
Thigh circumference. Overall, the average thigh circumference decreased by -3.45±4.50cm after the final treatment (p<0.001), -3.87±4.54cm at 1M FU (p<0.001), -2.63cm±3.27 at 3M FU (p<0.01) and -3.18±3.57cm (p<0.01) at 6M FU. Each thigh (i.e., left and right) decreased in circumference post-treatment (see Figure 1 for detailed results).
Hip circumference. Overall, the average hip circumference decreased post-treatment in comparison to baseline. The hip circumference decreased by -6.39±5.64cm after the final treatment (p<0.001), -7.22±5.17cm at 1M FU (p<0.001), -5.30±4.96cm at 3M FU (p<0.01) and -5.63±5.60cm at 6M FU (p<0.01).
The two-tailed paired T-tests, with significance set at 0.05, were calculated for the hip and thigh circumferences. The test showed that all differences were significant (hip circumference p=0.004, thigh circumference p=0.003). Peak circumference reduction of the hips and thighs was observed at 1-month post-treatment.
Abdomen and arm circumference
The abdomen (p<0.01) and arm (p>0.05) average circumferences decreased comparing baseline and the 6-months’ follow-up.
BMI and weight. The average body weight and BMI did not change significantly throughout the study (p>0.05).
Satisfaction and comfort. There was a high overall satisfaction rate after the treatments. Data showed 86 percent of subjects were satisfied with the appearance of the cellulite in the treatment area. Also, 82 percent of subjects reported improved skin laxity in the treated area. The average NRS comfort score was 2.8±2.3 (none to mild discomfort). There were no severe adverse events or side effects.

Discussion
Cellulite develops in different areas of the female body following puberty. The unappealing bulging fat pockets cause women to struggle with their appearance.27 The abdomen, thighs, hips, posterior arms, and buttocks may be affected. With the many treatment options available, non-invasive methods are highly sought after to improve the appearance and reduce the severity of the condition.
The blinded, independent evaluation of patient photographs judged the appearance of fat bulges, skin evenness, and laxity before and after treatments. In this study, overall cellulite severity improved from mild to moderate after treatments, and improvement of skin laxity in the treatment area was observed in the majority of the subjects.
Other research on non-invasive cellulite treatments reported mild-to-moderate reduction in severity after 6 to 20 RF or laser treatment,28,29 and between 6 to 12 sessions of mechanical and acoustic wave therapy.30,31 The evidence from this study suggests the combination of synergistic RF+TPE can cause long-term reduction of the signs of cellulite within four sessions in the thighs, hips, and abdomen. Nonetheless, an overall reduction in circumference was maintained even six months after the last treatment session. Eighty-six percent of patients expressed satisfaction with the improved appearance of the cellulite and 82 percent of subjects stated having firmer, less saggy skin in the treated area.
The cellulite-alleviating mechanisms of TPE include improved lymphatic and local vascular circulation, relieving oxidative stress, and counter-inflammatory effects. The RF component induces dermal remodeling by stimulating collagen repair and regeneration. Moreover, thermal energy penetrating the skin causes apoptotic lipolysis in adipocytes in the subcutaneous fat layer, thus causing fat pockets to shrink. Tissue tightening effects are achieved as septae become better organized.
The therapy is non-invasive, comfortable, and no adverse events occurred. There is no recovery period or downtime associated with this therapy, and it is suitable for patients with various skin types. A massage sensation can be felt with the pulsating invitations delivered by the handheld applicator, which is suitable for body parts.
The use of combined RF+TPE produces satisfactory results in a short period of time compared to some stand-alone, non-invasive modalities.32–34 This treatment method has demonstrated efficacy as an alternative to liposuction and further, in combination with HIFEM muscle stimulation, for body sculpting and enhancing tissue qualities. There is ongoing research on whether the RF+TPE study device may be beneficial to hasten the healing process of local bruising caused by injectable treatments for cellulite intervention,16,35 without causing further complications.




Conclusion
Combined TPE+RF is effective in reducing the characteristics of cellulite in multiple body parts. The treatment resulted in improved appearance and circumference reduction up to six months post-treatment. Therefore, the therapy may be useful as a non-invasive procedure to alleviate cellulite in postpubertal women.
References
- Arora G, Patil A, Hooshanginezhad Z, et al. Cellulite: Presentation and management. Journal of Cosmetic Dermatology. 2022;21(4):1393–1401.
- Araújo AR de, Soares VPC, Silva FS da, et al. Radiofrequency for the treatment of skin laxity: mith or truth. An Bras Dermatol. 2015;90(5):707–721.
- Zerini I, Sisti A, Cuomo R, et al. Cellulite treatment: a comprehensive literature review. Journal of Cosmetic Dermatology. 2015;14(3):224–240.
- Omi T, Sato S, Kawana S. Ultrastructural assessment of cellulite morphology: clues to a therapeutic strategy? Laser Ther. 2013;22(2):131–136.
- Tokarska K, Tokarski S, Woźniacka A, et al. Cellulite: a cosmetic or systemic issue? Contemporary views on the etiopathogenesis of cellulite. Postepy Dermatol Alergol. 2018;35(5):442–446.
- Luebberding S, Krueger N, Sadick NS. Cellulite: An Evidence-Based Review. Am J Clin Dermatol. 2015;16(4):243–256.
- Piérard GE, Nizet JL, Piérard-Franchimont C. Cellulite: from standing fat herniation to hypodermal stretch marks. Am J Dermatopathol. 2000;22(1):34–37.
- Emanuele E. Cellulite: advances in treatment: facts and controversies. Clin Dermatol. 2013;31(6):725-730.
- Hexsel DM, Dal’forno T, Hexsel CL. A validated photonumeric cellulite severity scale. J Eur Acad Dermatol Venereol. 2009;23(5):523–528.
- Emanuele E, Bertona M, Geroldi D. A multilocus candidate approach identifies ACE and HIF1A as susceptibility genes for cellulite. Journal of the European Academy of Dermatology and Venereology. 2010;24(8):930–935.
- Emanuele E, Minoretti P, Altabas K, et al. Adiponectin expression in subcutaneous adipose tissue is reduced in women with cellulite. Int J Dermatol. 2011;50(4):412–416.
- Leszko M. Cellulite in menopause. Prz Menopauzalny. 2014;13(5):298–304.
- Uitto J. The role of elastin and collagen in cutaneous aging: intrinsic aging versus photoexposure. J Drugs Dermatol. 2008;7(2 Suppl):s12–16.
- Uitto J, Li Q, Urban Z. The complexity of elastic fibre biogenesis in the skin–a perspective to the clinical heterogeneity of cutis laxa. Exp Dermatol. 2013;22(2):88–92.
- de la Casa Almeida M, Suarez Serrano C, Rebollo Roldán J, et al. Cellulite’s aetiology: a review. J Eur Acad Dermatol Venereol. 2013;27(3):273–278.
- Kaufman-Janette J, Joseph JH, Kaminer MS, et al. Collagenase Clostridium Histolyticum-aaes for the Treatment of Cellulite in Women: Results From Two Phase 3 Randomized, Placebo-Controlled Trials. Dermatol Surg. 2021;47(5):649–656.
- Kaufman JD, Fesmire CC, Petrella RA, et al. High-Frequency Irreversible Electroporation Using 5,000-V Waveforms to Create Reproducible 2- and 4-cm Ablation Zones—A Laboratory Investigation Using Mechanically Perfused Liver. Journal of Vascular and Interventional Radiology. 2020;31(1):162–168.e7.
- Duncan D, Chilukuri S, Kent D, et al. Non-Invasive Alternatives for Liposuction. IntechOpen. 2022.
- Kinney BM, Kanakov D, Yonkova P. Histological examination of skin tissue in the porcine animal model after simultaneous and consecutive application of monopolar radiofrequency and targeted pressure energy. J Cosmet Dermatol. 2020;19(1):93–101.
- Fritz K, Salavastru C, Gyurova M. Clinical evaluation of simultaneously applied monopolar radiofrequency and targeted pressure energy as a new method for noninvasive treatment of cellulite in postpubertal women. J Cosmet Dermatol. 2018;17(3):361–364.
- Fritz K, Salavastru C, Gyurova M. Reduction of abdominal skin laxity in women postvaginal delivery using the synergistic emission of radiofrequency and targeted pressure energies. J Cosmet Dermatol. 2018;17(5):766–769.
- Page-McCaw A, Ewald AJ, Werb Z. Matrix metalloproteinases and the regulation of tissue remodelling. Nat Rev Mol Cell Biol. 2007;8(3):221–233.
- Duncan DI, Kreindel M. Basic Radiofrequency: Physics and Safety and Application to Aesthetic Medicine. In: Lapidoth M, Halachmi S, eds. Aesthetic Dermatology. Vol 2. S. KARGER AG; 2014:1–22.
- Christ C, Brenke R, Sattler G, et al. Improvement in skin elasticity in the treatment of cellulite and connective tissue weakness by means of extracorporeal pulse activation therapy. Aesthet Surg J. 2008;28(5):538–544.
- Raza A, Harwood A, Totty J, et al. Extracorporeal Shockwave Therapy for Peripheral Arterial Disease: A Review of the Potential Mechanisms of Action. Annals of Vascular Surgery. 2017;45:294–298.
- Schaupper M, Jeltsch M, Rohringer S, et al. Lymphatic Vessels in Regenerative Medicine and Tissue Engineering. Tissue Eng Part B Rev. 2016;22(5):395–407.
- Friedmann DP, Vick GL, Mishra V. Cellulite: a review with a focus on subcision. Clin Cosmet Investig Dermatol. 2017;10:17–23.
- Wanitphakdeedecha R, Sathaworawong A, Manuskiatti W, et al. Efficacy of multipolar radiofrequency with pulsed magnetic field therapy for the treatment of abdominal cellulite. Journal of Cosmetic and Laser Therapy. 2017;19(4):205–209.
- Harth Y. Painless, safe, and efficacious noninvasive skin tightening, body contouring, and cellulite reduction using multisource 3DEEP radiofrequency. J Cosmet Dermatol. 2015;14(1):70–75.
- Nassar AH, Dorizas AS, Shafai A, et al. A randomized, controlled clinical study to investigate the safety and efficacy of acoustic wave therapy in body contouring. Dermatol Surg. 2015;41(3):366–370.
- Hexsel D, Camozzato FO, Silva AF, et al. Acoustic wave therapy for cellulite, body shaping and fat reduction. J Cosmet Laser Ther. 2017;19(3):165-173.
- Duncan D. Synergy of Monopolar Radiofrequency Heating and Targeted Pressure Energy as an Innovative Approach to Cellulite Reduction. AJBSR. 2021;12(1):83–85.
- Duncan DI. Combination treatment for buttock and abdominal remodeling and skin improvement using HIFEM procedure and simultaneous delivery of radiofrequency and targeted pressure energy. J Cosmet Dermatol. Published online October 22, 2021.
- Duncan DI, Busso M. Effectiveness of combined use of targeted pressure energy, radiofrequency, and high-intensity focused electromagnetic fields to improve skin quality and appearance of fat and muscle tissue in different body parts. Journal of Cosmetic Dermatology. 2023 Jan;22(1):200–205.
- Gold MH. Treatment of bruising after injection to reduce cellulite. Journal of Cosmetic Dermatology. 2023 Jan;22(1):55–63.