Scott M. Dinehart, MD, Arkansas Skin Cancer Center, Little Rock, Arkansas; Matt Graham, BS, University of Arkansas for Medical Sciences, Little Rock, Arkansas; Ann Maners, MD, Central Arkansas Radiation Therapy Institute, Little Rock, Arkansas
Disclosure: The authors report no relevant conflicts of interest.
Abstract
Objective: To profile 16 patients with widespread and resistant actinic keratoses (AKs) treated with radiation therapy. Design: Chart review and phone interviews of 16 patients who were treated with radiation therapy between 2003 and 2010. Setting: A specialized dermatological practice primarily treating patients with skin cancer. Participants: The study population at the time of treatment was aged 70 to 87 with a mean age of 79.6 years and included 14 men and two women. Measurements: Patients were followed at two weeks and six months after treatment to assess clinical outcome. All adverse effects were recorded. Patients were contacted for phone interview to assess patient satisfaction after treatment. Results: Patients all had significant reduction of AKs in the radiation field with a majority (90%) reporting they were “very satisfied” with their treatment outcome. Of 16 patients at two weeks post-treatment, 13 had complete clinical resolution of their AK after radiation therapy. Three of 16 patients had significant reduction (50–99%) in AK in the treatment field. Patients reported improved quality of life, a reduced need for frequent clinic visits, and long-term remission from the development of new AKs within the treatment field. Conclusion: Patients meeting suggested specific criteria developed by the authors may be treated successfully with radiation therapy with good outcomes at six-month follow up and high levels of patient satisfaction. (J Clin Aesthet Dermatol. 2011;4(7):47–50.)
Actinic keratoses (AKs) are premalignant clinical lesions that correlate histologically to atypical keratinocytes within the epidermis. They are very common and account for an estimated 5.2 million patient visits to dermatologists in the United States each year.[1] The risk of progression of AKs to cutaneous squamous cell carcinoma (SCC) is well documented. Some clinicians suggest that AKs can go untreated because the risk of progression to SCC is low, but most clinicians elect to treat each AK because it is not currently possible to predict which AK will progress to SCC.
Many effective treatments for AKs are available. While almost all patients will respond to one or more standard therapies, there is a small subgroup of patients who are resistant to conventional treatment. The authors describe 16 patients with widespread AKs who failed numerous standard therapies and were eventually treated with radiation therapy. They also present criteria that are useful to identify patients with AKs who can be treated effectively and safely with this modality.
Patients
Electronic medical records (EMR) and paper charts of patients treated with radiation therapy were reviewed from 2003 to 2010. Patients who had been treated primarily for AK were selected. Additionally, patients who had superficial SCC or basal cell carcinoma (BCC) and the radiation field expanded during treatment to encompass surrounding AK were included. All patients had clinical evidence of AK with histological confirmation. Patients were excluded if they were treated for invasive skin cancers. Patients typically had widespread treatment-resistant AK and had attempted multiple treatment modalities. Patients were followed up two weeks after their final radiation treatment and again at six months. Primary outcomes measured were complete clinical resolution (100%), significant reduction (50–99%), and poor reduction of AK (0–49%).
Results
Fourteen men and two women were included in this review with a mean age at treatment of 79.6 years. Four patients had an indication for radiotherapy and had the field expanded to encompass their surrounding AK. Twelve patients were treated primarily for AK.
Patients were treated with fractionated dosages of radiation therapy over 4 to 6 weeks five days per week. The cumulative dosages of radiation ranged from 40 to 60Gy utilizing primarily electrons and photons. The initial visit with the radiation oncologist required approximately one hour and all subsequent visits for treatment were 5 to 20 minutes in duration.
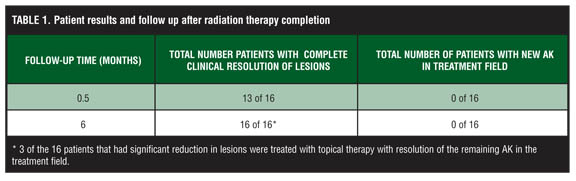
Of 16 patients, 13 had complete clinical resolution of the AK within the treatment field at two weeks post-radiation treatment. Three of the 16 patients had significant reduction (50–99%) in the number of AK within the treatment field (Table 1). These patients were treated with topical therapy and all had clinical resolution of their AK.
{kind=link}
Patients were contacted by phone for interview and feedback from January 2010 to March 2010. Ten of the 16 patients were interviewed, three were deceased, and three could not be reached. Patients were asked, “Do you agree or disagree that radiation therapy has improved your quality of life?” They were given the option of responding, “totally agree, partially agree, neither agree or disagree, partially disagree, totally disagree.” Nine of the 10 patients responded, “totally agree,” and one responded, “totally disagree.” The patient responding, “totally disagree,” felt that although the lesions initially cleared they were beginning to reappear approximately one year after treatment. Patients also reported they were very satisfied with the cosmetic results of their treatment as well as the reduction in the need for frequent office visits. Other patient feedback included, “very pleased with result,” “I don’t get lesions in radiation field, but I do in other places.” Most patients reported they have remained free of new lesions in the treatment field or have had very minimal recurrences.
Patients generally tolerated radiotherapy very well. Some side effects seen were dose-dependent alopecia, erythema, hypo/hyperpigmentation, and crusting. One patient experienced skin breakdown on the posterior aspect of his scalp requiring galeal flap reconstruction.
Figure 1 and Figure 2 illustrate a 70-year-old man with a history of SCC in situ and multiple refractory. The patient failed treatment with electrodessication and curettage, cryotherapy, 5-fluorouracil, and imiquimod. He was treated for four weeks with radiation therapy and was clinically free of AK in the treatment field three months after therapy.
{kind=link}
{kind=link}
Discussion
The trend in recent years has been the development of AK treatments that not only treat a single lesion, but also treat surrounding and adjacent skin that is subclinically damaged. The hope is that this type of therapy might be more likely to result in long-term remissions. Additionally, a goal of this type of therapy is to prevent the development of clinically atypical lesions in the affected field. The concept of field cancerization and the desire to treat entire areas or fields of damage has driven the development of novel treatments for AKs, such as imiquimod cream, diclofenac gel, and photodynamic therapy. 5-flourouracil cream has been used for decades for this very purpose. Our use of radiation as field therapy for treatment of widespread, resistant AKs is consistent with this concept and has the same goals and endpoints. Radiation therapy for AKs is rarely reported and the reports are limited to two case reports.[2,3]
This study shows that radiation therapy is an effective therapy for a select group of patients with resistant widespread AKs. The idea of utilizing radiation therapy as an effective treatment stemmed from years of observing how well irradiated skin surrounding treated nonmelanoma skin cancer (NMSC) appeared. Often the area surrounding the primary lesion treated had AKs, which resolved and often remained without recurrence for long periods of time versus adjacent skin not in the treatment field. This led to the consideration of using radiotherapy for primary treatment of AK.
Radiotherapy has many advantages in treating AK. Large fields of damaged skin can be treated at the same time. The AKs in addition to subclinically damaged skin, hyperkeratotic AK, and NMSC may be treated simultaneously. The quality of life in patients may be dramatically improved and the cosmetic result is typically excellent. In the experience of the authors, after the radiation therapy regimen is completed, the frequency of office visits for treatment and surveillance of AK typically decreases accordingly with skin improvement. Office visits contribute to the vast majority of direct costs for AK treatment. Lost workdays accounted for the largest indirect cost related to AKs. Lost caregiver workdays also substantially contribute to indirect costs related to AKs.[4] A decrease in office visits may offset some of the high costs of utilizing radiation therapy.
Radiation therapy with electrons and photons allows for predictable cure rates and penetration of skin depth.[5] Minimal wound care is required after treatment. Morbidity of the procedure is limited and the inflammatory reaction is typically less severe than with 5-fluorouracil, imiquimod, or other therapies.
Some disadvantages of radiotherapy include high cost, time commitment, limited access to radiation therapy centers, and decreased vascularity in treatment field. The side effect profile is minimal, but includes radiation dermatitis, hypo/hyperigmentation, telangiectasia, and dose-dependent alopecia. There is also a small risk of developing a radiogenic secondary malignancy. The risk of developing secondary malignancy after treatment of skin cancers with radiation therapy, which utilizes similar doses of radiation exposure, is very low. Additionally, the latency period for the development of cancer varies from 4 to 40 years with a median of 24.5 years.[5]
Treating these 16 patients as well as many others over the past 15 years, the authors feel criteria for treating AK with radiation therapy should be outlined (Table 2).
{kind=link}
Radiation therapy for AK should be a rare, last-resort treatment option for patients with extremely difficult-to-manage AK. Patients being considered should meet the criteria in Table 2. Both of the major criteria should be met. Minor criteria should be considered in the selection of patients for radiation therapy. The patient should be 70 years of age or greater to reduce the possibility of developing radiogenic secondary malignancy. However, a patient who is less than 70 years old and in poor health may also be considered. Conservative treatment modalities should be attempted and failed before considering using radiotherapy. Some patients will have indications for radiotherapy for skin lesions in an area where multiple AKs coexist. In this scenario, it may be beneficial for the patient to have the radiation field expanded to encompass these areas. As always, the patient’s health status is critical and patients in fair-to-poor health are more suited for radiotherapy versus surgical modalities. It is also prudent to consider the quality of life of each patient when considering radiation therapy. Location for treatment should be limited to the face and scalp. The authors feel that radiation therapy to these areas has been most beneficial and has had the best outcomes. In a review of 1,188 patients irradiated for cutaneous neoplasms, poorer cosmetic outcomes on the arms, legs, neck, and trunk in addition to higher rates of radiation dermatitis in these areas versus the head were demonstrated.6 For many patients, other therapies require considerable time commitment and cause significant morbidity and cosmetic disfigurement. Radiation therapy may offer long-term remission from AK, minimal morbidity, and excellent cosmetic outcomes.
This case review is limited by the small number of participants and limited follow up. Further studies in the future should include longer term follow up or comparison to other treatment modalities.
Summary
SCC is a potentially life-threatening sequalae of untreated AKs. Treatment of widespread AK will decrease new development of new AKs and SCC, thereby decreasing overall morbidity and mortality. Radiotherapy is an often overlooked treatment modality and when patients are selected appropriately, provides an excellent therapeutic option.
References
1. Warino L, Tusa M, Camacho F, Teuschler H, et al. Frequency and cost of actinic keratosis treatment. Dermatologic Surg. 2006;32(8):1045–1049.
2. Pipitone MA, Gloster HM. Superficial squamous cell carcinomas and extensive actinic keratoses of the scalp treated with radiation therapy. Dermatologic Surgery. 2006; 32:756–759.
3. Barta U, Gräfe T, Wollina U. Radiation therapy for extensive actinic keratosis. Eur Acad Dermatol Venereol. 2000;14:293–295.
4. Neidecker MV, Davis-Ajami ML, Balkrishnan R, Feldman SR. Pharmacoeconomic considerations in treating actinic keratosis. Pharmacoeconomics. 2009;27(6):451–464.
5. Goldschmidt H, Panizzon RG. Modern Dermatologic Radiation Therapy. New York: Springer; 1991.
6. Caccialanza M, Piccino R, Beretta M, et al. Results and side effects of dermatologic radiotherapy: a retrospective study of irradiated cutaneous epithelial neoplasms. J Am Acad Dermatol. 1999;41(4):589–594.