 J Clin Aesthet Dermatol. 2021;14(8):E76–E85.
J Clin Aesthet Dermatol. 2021;14(8):E76–E85.
by Niamh Corduff, MBBS, FRACS; Jeng Feng CHEN, MD; Ya Hui CHEN, MD; Ho Sung CHOI, MD; Kate GOLDIE; Yui LAM, MBBS; Nyoman Indra LESTHARI; Ting Song LIM, MD; Suzanna LUO; Arnelle QUIAMBAO, MD; Tuck Wah SIEW, MBBS; Fang Wen TSENG, MD; and Yates Y. Y. CHAO, MD
Dr. Corduff is with the Cosmetic Refinement Clinic in Geelong, Australia. Dr. J. F. Chen is with Tri-Service General Hospital in Taipei, Taiwan. Dr. Y. H. Chen is with YaSkin Dermatology Clinic in Kaohsiung, Taiwan. Dr. Choi is with PIENA Aesthetic Medical Clinic in Gangnam, Seoul, South Korea. Ms. Goldie is with European Medical Aesthetics in London, England. Dr. Lam is with the Skin Care Clinic in Tsim Sha Tsui, Hong Kong. Lesthari is with Sano Clinic in Denpasar, Bali, Indonesia. Dr. Lim is with Clique Clinic in Petaling Jaya, Selangor, Malaysia. Ms. Luo is with Medical Aesthetics 360 in Hurstville, New South Wales, Australia. Dr. Quiambao is with YouPlus Intelligent Aesthetic Clinic in Taguig City, the Philippines. Dr. Siew is with Radium Medical Aesthetics in Singapore. Dr. Tsend is with Milano Aesthetic Clinic in Taoyuan, Taiwan. Dr. Chao is with the CHAO Institute of Aesthetic Medicine in Taipei, Taiwan.
FUNDING: Funding for the preparation of this manuscript was provided by Merz Asia Pacific Pte. Ltd. to Dr. Shawna Tan, Medical Writers Asia.
DISCLOSURES: All authors received an honorarioum for attendance at the consensus meeting.
ABSTRACT: Background. Several usage guidelines for calcium hydroxylapatite (CaHA), a dermal filler material, exist for non-Asian patients, making it necessary to determine whether their findings and consensuses are applicable to Asian patients who have distinct anatomies, cultural preferences, and aesthetic requests.
Objective. We sought to develop a Pan-Asian consensus on CaHA use in skin biostimulation, contouring, and combination treatments for face and body indications.
Methods. A survey on CaHA usage for contouring and biostimulation indications in Asian patients was conducted, followed by discussions to establish consensus statements and topics for examination.
Results. Several aspects of facial shaping and contouring or skin biostimulation with CaHA were agreed on, including that dilution is not a key consideration, that microfocused ultrasound with visualisation precedes CaHA in same day or session treatments, and that cannulas should be used. Among the many agreements on interventions in specific facial and body areas, there were also disagreements due to the diverse Asian patient presentations, requests, and access to tools or products; for example, CaHA should be placed in the interfascial layer for temple contouring, CaHA should not be injected directly into the infraorbital area for safety, and diluted CaHA should be injected subdermally for nonfacial or whole-face biostimulation and contouring.
Conclusion. Our disagreements highlight the diversity of Asian facial morphotypes and desired aesthetic outcomes and underscore the need for customized aesthetic strategies to accommodate the heterogeneity of Asian anatomies, cultural preferences, and aesthetic ideals. Establishing consensus statements on critical aspects of Asian patient considerations, efficacy and safety, is crucial. This document provides strategic guidance on the use of classic, diluted CaHA for biostimulation or undiluted Radiesse®(+) (Merz Pharma GmbH & Co. KGaA, Frankfurt, Germany) for lifting and contouring to ensure consistent CaHA delivery for successful patient outcomes.
Keywords: Asian, calcium hydroxylapatite, consensus statement, dermal fillers
Dermal fillers have become one of the most popular clinical aesthetic treatments, with 2.6 million injections delivered in 2018 in the United States.1 Their popularity is partly due to their less-invasive nature and shorter downtime compared to surgical procedures. In 2018, the most frequently-used fillers were hyaluronic acid (HA); calcium hydroxylapatite (CaHA), known commercially as Radiesse® (Merz Pharma GmbH & Co. KGaA, Frankfurt, Germany); and poly-L-lactic acid fillers.
Radiesse contains 30% synthetic CaHA suspended in a 70% aqueous sodium carboxymethylcellulose gel matrix.2 CaHA occurs naturally in human bone and teeth; is progressively and naturally metabolized and excreted; and in the injectable filler, the CaHA forms uniform 25- to 45-um microspheres. Its gel component allows it to immediately and linearly (1:1) correct volume deficits upon injection and is eventually resorbed. This brings CaHA microspheres into direct contact with tissues to stimulate collagenesis, sustain volumization, and avoid the need for overfilling.3 In its nonlidocaine formulation, CaHA is used for facial definition, contouring, and skin tightening in both undiluted, minimally-diluted, and hyperdiluted formats. A recent variant, Radiesse®(+) (Merz Pharma GmbH & Co. KGaA), contains 0.3% integral lidocaine hydrochloride for improved pain control4 and is now approved by the United States Food and Drug Administration (FDA) and is CE-certified in Europe. CaHA is an ideal soft-tissue filler as it is consistently effective and does not migrate or cause long-term discomfort.5 For example, 81% of patients with jawline CaHA injections in one study experienced “improved” to “very much improved” contour restoration and significantly improved marionette lines at one year postinjection,6 while studies with Radiesse®(+) in temples7 and hands8 proved its safety and efficacy. Twenty patients receiving jawline Radiesse®(+) injections had statistically-significant volume restoration and improved appearances,9 thus supporting rheological studies showing that Radiesse®(+) produces a similar degree of volume restoration to that of CaHA.10 To date, however, few investigations have been published on Radiesse®(+), especially in Asian patients.11 Off-label usage of soft-tissue fillers is now common practice worldwide,12 especially in the Asia-Pacific (APAC) region, where physicians frequently use CaHA for both face and body contouring, augmentation, volumization, and biostimulation. Expert physicians who routinely treat Asian patients have innovated and mastered filler techniques and strategies that are sought out by those less experienced. This knowledge includes the use of combination modalities, such as other fillers, energy-based devices [e.g. fractional lasers, microfocused ultrasound with visualisation (MFU-V) (Ultherapy®; Merz Pharma GmbH & Co. KGaA)], and neurotoxins.
Several CaHA uage guidelines exist at this time for non-Asian patients,13–15 making it necessary to determine whether their findings and consensuses are applicable to Asian patients, who have distinct anatomies, cultural preferences, and aesthetic requests.16 Thus, in May 2019, 12 leading plastic surgeons, dermatologists, and aesthetic physicians (“Experts”) from Europe and APAC convened to discuss CaHA usage in Asian patients. Specifically, these clinicians aimed to develop a Pan-Asian consensus for the optimal CaHA dilution ratio and injection technique for skin biostimulation and contouring and for combining MFU-V with CaHA for face and body indications.
Methods
Twelve Experts first completed an electronic survey (SurveyMonkey, Inc., San Mateo, CA, USA) to document their usage of CaHA for contouring and biostimulation indications in Asian patients. These results were debated during the face-to-face meeting to establish statements for subsequent consensus voting led by two experienced moderators.
For these discussions, the following points were considered:
- Unless stated, CaHA is used undiluted
- Radiesse®(+) was unavailable at the time of the meeting in Taiwan
- Dilution was defined solely as the use of a delivery vehicle for the required product dose
- Unless stated, diluted CaHA refers to a 1:1 dilution (product:diluent) ratio
- Dose was defined as the absolute total quantity of product delivered (regardless of volume of diluent used); therefore, when it is stated that 1.5 mL of diluted CaHA is injected, this means that a total volume of 3 mL is injected, inclusive of diluent and 1.5 mL of CaHA
- Hyperdilution was defined as the use of diluent at a ratio of least 1:2 ratio
- Minimal dilution was defined as the use of at least 0.3 mL of diluent per 1.5 mL of filler
- When calculating product quantities, either the patient’s hand surface area or a 100-cm2 area qualified as a unit of measurement
- The décolletage was not considered part of the neck
For contouring with CaHA, common indications in the upper face (temple and forehead), mid-face (malar and zygoma, submalar and subzygoma, and infraorbital region) and lower face (perioral area, jawline and chin) were considered. For biostimulation indications, skin biostimulation of the face and body (hands, elbows, abdomen and neck) were considered. Treatment factors discussed included the most common dilution (e.g., 1:1, undiluted), injection plane (e.g., subdermal, supraperiosteal, interfascial), injection technique (e.g., microbolus, bolus, anaesthetics, hydrodissection), injection tools and size of tools, most common CaHA dose, injection entry points, combination treatments for biostimulation, and warnings and additional considerations.
A consensus was reached when all Experts agreed with a statement, whereas a strong agreement required 81% to 99% of Experts to concur. Moderate agreement occurred when 61% to 80% of Experts agreed, while no agreement occurred when up to 60% of Experts agreed. These lower levels of agreement represented a variety of patient profiles and geographical coverage, resulting in nuances that benefit injectors wishing to expand or deepen their practices, and thus warranted discussion. Not all voting totaled 100% due to overlaps in considerations or procedures; for example, rather than choosing between either needles or cannulas, both may be used depending on a patient’s presentation or treatment request.
Results
Demographics. The Experts consisted of plastic surgeons, aesthetic general practitioners, and dermatologists, most of whom had used CaHA for facial contouring and skin biostimulation for five to 10 years and now routinely combine CaHA with MFU-V for lower-, mid- and upper-face contouring (Supplementary Figure 1). The involved physicians practice in Hong Kong, Malaysia, Taiwan, South Korea, Indonesia, the Philippines, Australia, and the United Kingdom. For body skin biostimulation, most Experts reported having used CaHA for two to five years but do not routinely combine CaHA and MFU-V (data not shown).

Statements of agreement or consensus on contouring and biostimulation with CaHA. Generally, when performing facial shaping and contouring or skin biostimulation in Asian patients, the Experts agreed on several general considerations and statements (Table 1) including that most patients present in their early-30s for aging-related face contouring and between 30 to 50 years of age for biostimulation indications.

Consensus was also reached on all specific aspects of CaHA use discussed (Table 2). The Experts emphasized that dilution was not a critical consideration and should not be confused with dosage. With respect to same-day treatment sequence, all Experts perform MFU-V before injecting CaHA if both procedures are to be completed in a single session. Most Experts adopt this treatment sequence due to concerns about contamination, CaHA migration or deformation by the MFU-V transducer, and alteration of tissue planes by filler injection prior to MFU-V treatment. Unless specified in the subsequent sections, most Experts use 25-gauge cannulas while only a few use 22-gauge cannulas. For biostimulation, the Experts varied between using one syringe (i.e., 1.5 cc) for the whole face or the whole neck to using one syringe per contralateral face or neck. As a practical guide to estimate dosage for the biostimulation of large treatment areas, the patient’s hand surface area was regarded as equivalent to one syringe of filler. The most commonly used dilution ratio was 1:1, with both lidocaine and normal saline frequently employed for filler dilution.
The only consensus achieved was of using cannulas to inject CaHA between the temporoparietal fascia and deep temporal fascia (interfascial layer) (Table 3) for temple contouring. A majority of the Experts dilute 1:1 for superficial temple contouring and inject 0.5 to 1.0 cc per temple, while a minority inject less than 0.5 cc of CaHA per temple. Some Experts use a zygoma entry point with 23-gauge cannulas, while the remainder enter via the temporal crest, and diluted CaHA is placed in the interfascial layer. For deep temple contouring, the majority of Experts also perform additional supraperiosteal injections of 0.5 to 1.0 cc of undiluted CaHA-accumulated micro-boluses per temple, while a minority inject in an accumulated bolus of less than 0.5 cc per temple. For patient safety, new injectors should proceed cautiously in this area. Figure 1 provides an expected aesthetic outcome following CaHA injection for temple contouring.


Consensus was reached on using cannulas for the injection of struts of CaHA along the jawline (Table 4). Most Experts would insert their cannulas in the subcutaneous plane to inject struts or microboluses on the mandible. The majority also agreed that CaHA should be combined with MFU-V to optimize contouring and lifting of the lower face, submentum, and jawline. In this context, half of the Experts would use 22-gauge cannulas, while the remainder use 25-gauge cannulas, and the injected dose varies between less than 0.5 cc (25% of Experts), 0.5 to 1 cc (58%), and more than 1 cc (17% ) per contralateral jawline. Where Radiesse®(+) was available, 58% of Experts would use it without further dilution. Approximately 42% of Experts would use minimally-diluted CaHA if Radiesse®(+) was unavailable. For combination therapy of the jawline, most Experts perform all procedures on the same day.
No consensus was reached for any aspect of chin contouring (Table 5); however, the majority of Experts agreed that filler should be injected with needles as micro-boluses supraperiosteally and 67% would use undiluted CaHA. Few Experts would use a 25-gauge cannula or place it in multiple anatomical planes. Most of the Experts (7/12 physicians) advocated using more than 1 cc of CaHA. Figure 2 demonstrates the potential aesthetic outcomes in the chin following CaHA injection.
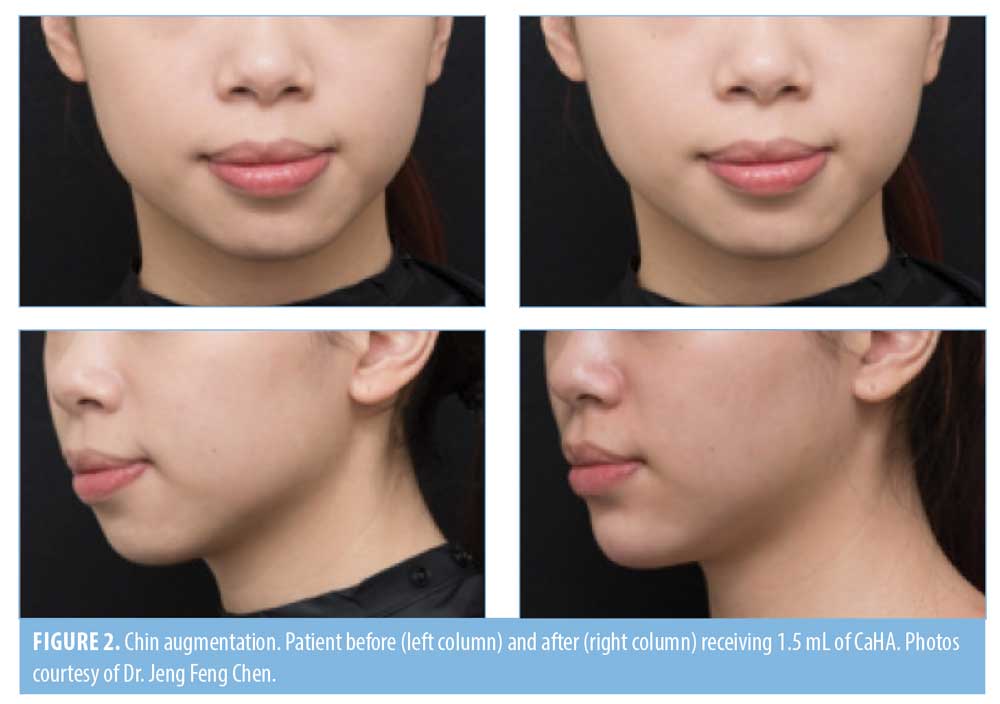

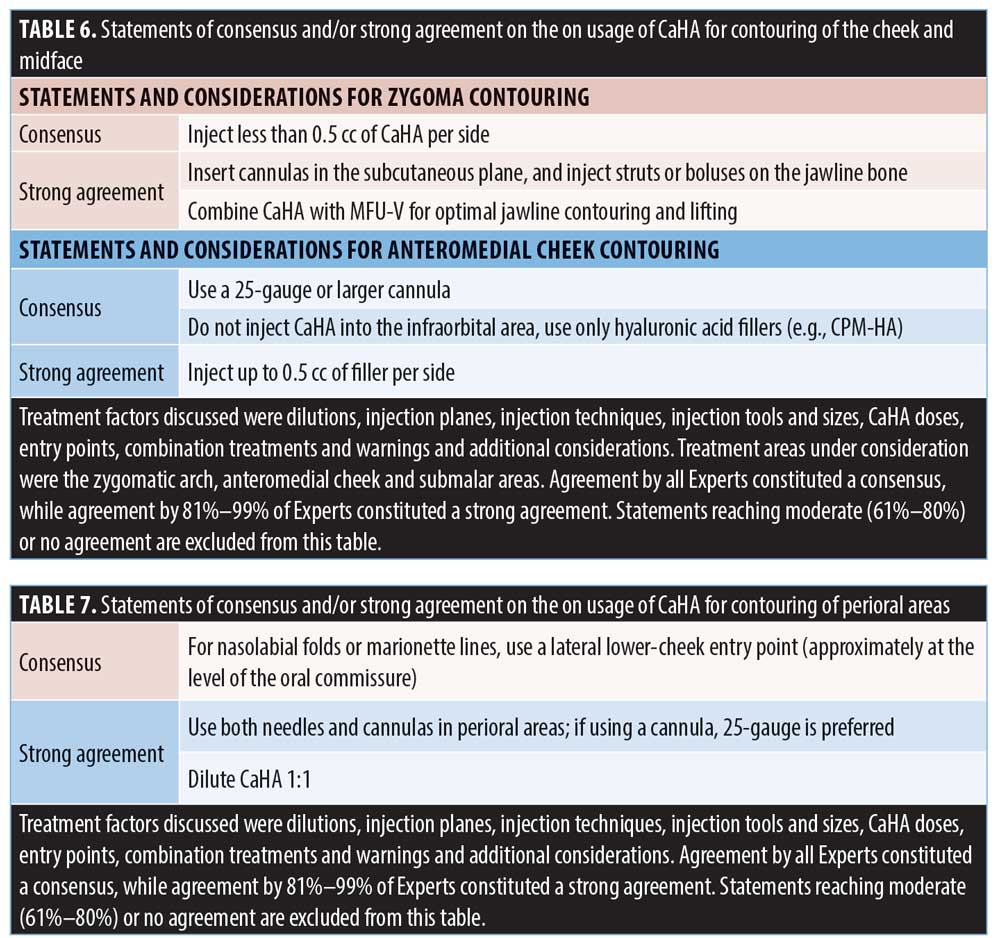
Figure 3 demonstrates the segregation of the cheek into the zygoma, anteromedial cheek, and submalar regions for the purposes of these discussions. Only 50% of Experts would contour the zygoma; however, if required, all Experts would inject filler in lower quantities (< 0.5 cc) in the contralateral face (Table 6). The zygomatic arch is never treated superficially or subcutaneously. Instead, 75% of Experts would inject filler supraperiosteally with a needle, in multiple sites along the banana-shaped zygomatic arch. Where available, many Experts (7/12 physicians) use Radiesse®(+) without further dilution. Fewer than half of Experts use needles (27-gauge), and, of the one-third who use cannulas, half use 22-/23-gauge cannulas, while the rest use 25-gauge cannulas. One quarter (25%) of Experts create a cannula entry point laterally over the zygomatic arch, 8% create an entry point below the malar eminence, and all Experts deposit the filler while moving cannulas back-and-forth continuously.

The Experts agreed that cannulas should be used in the anteromedial cheek area (Table 6). Most Experts inject less than 0.5 cc of filler per contralateral cheek, while the rest inject 0.5 to 0.99 cc. All Experts use 25-gauge or larger cannulas. Entry points are usually created below the malar eminence and along a vertical line, transecting the lateral orbital rim. For contouring, most Experts would use undiluted Radiesse®(+) if available, while the remaining would use undiluted or minimally diluted CaHA. All Experts who perform biostimulation with fillers would dilute CaHA 1:1. For safety reasons, consensus was reached to avoid CaHA injections directly into the infraorbital area.
For the purposes of these discussions, the perioral area included the nasolabial folds and marionette lines. In these areas, all Experts use and insert cannulas through a lateral lower-cheek entry point (approximately at the level of a line drawn horizontally from the oral commissure) and advance toward the treatment area at an angle from lateral to medial, although half would also enter via the tail of marionette lines (Table 7). Experts dilute CaHA 1:1 for delivery using both needles (86%) and cannulas (71%). The rest dilute CaHA minimally. No agreement was reached on dosage for the perioral area, as 56% inject less than 0.5 cc, 20% inject 0.5 to 0.99 cc, and 30% inject 1 to 1.5 cc of filler.
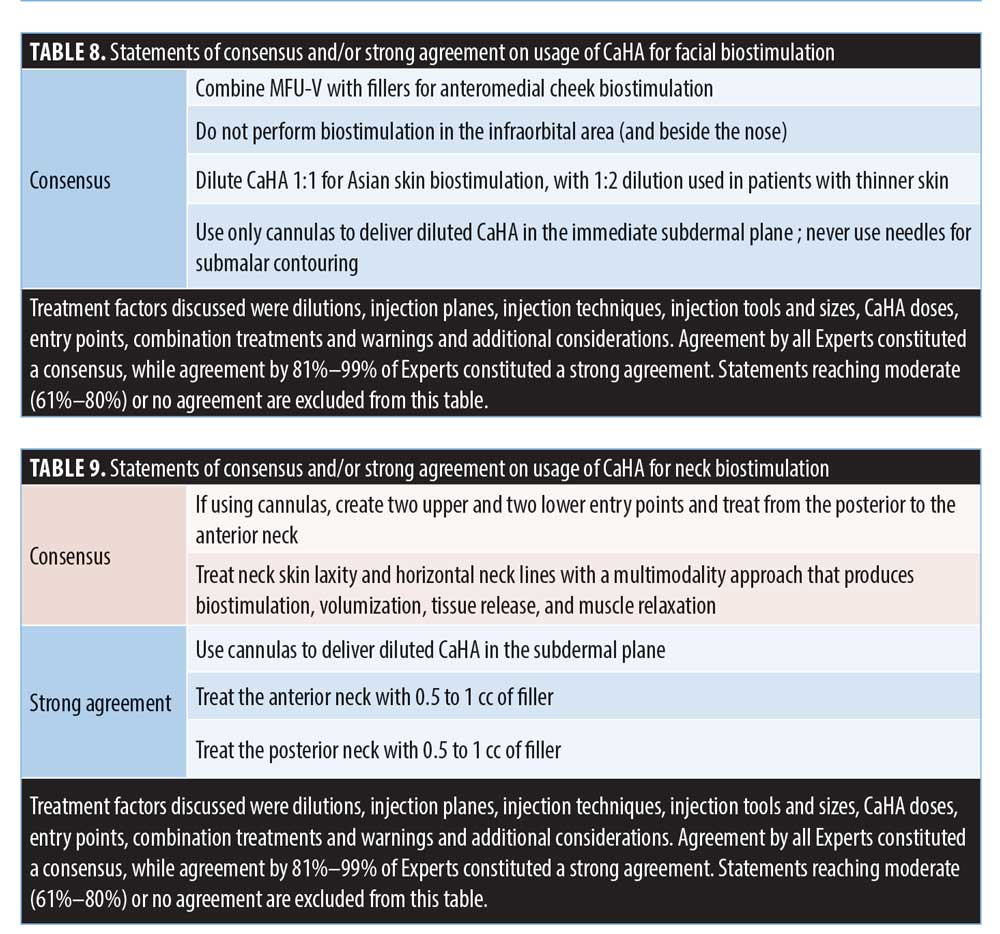
Facial biostimulation is most commonly performed in the submalar region. Consensus was obtained on avoiding biostimulation with CaHA in the infraorbital area for safety reasons. Most Experts inject between 0.5 and 0.99 cc per contralateral submalar for whole-face skin biostimulation and pore size improvement. It should be noted that pores exist mostly over the anteromedial cheeks and are less prominent in submalar areas. All Experts commonly dilute CaHA 1:1 for Asian skin biostimulation, with 1:2 dilution used in patients with thinner skin. All Experts use only cannulas to deliver diluted CaHA in the immediate subdermal plane (Table 8); needles are never used for submalar contouring. Most Experts use minimally diluted CaHA for whole-face contouring. Figure 4 demonstrates the potential aesthetic outcomes following facial biostimulation with diluted CaHA.

The anterior neck was defined as the area between the mandible, sternum, anterior clavicles, and anterior border of the bilateral sternocleidomastoid muscle. The posterior neck was defined as the area posterior to the sternocleidomastoid muscle. Most (86%) Experts prefer to use cannulas for neck biostimulation. The Experts agreed that, for biostimulation, cannulas are traversed across the neck from the posterior to anterior areas in the subdermal plane, superficial to the platysma muscle. The most effective treatment for neck skin laxity and horizontal necklines involves a multimodality approach that produces biostimulation, volumization, tissue release, and muscle relaxation (Table 9). Most use 0.5 to 1 cc of filler for both the anterior and posterior neck. A minority of the Experts use 1 to 1.5 mL of filler. The majority (55%) of the Experts use diluted CaHA; 36% will hyperdilute to a ratio between 1:1 to 1:2 and 9% will hyperdilute to 1:4.
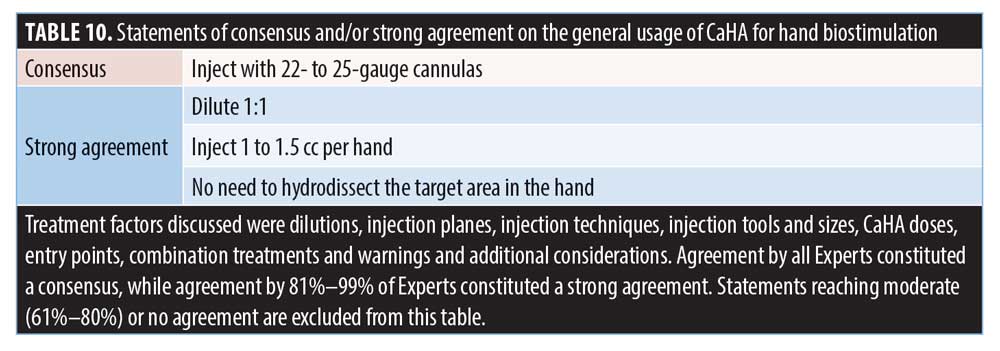
All Experts use 22- to 25-gauge cannulas, 82% use diluted CaHA, 9% use 1:2 hyperdiluted CaHA, and 9% use higher dilutions (Table 10). Most Experts inject 1 to 1.5 cc per hand and do not hydrodissect, whereas just 17% inject 0.5 to 1 cc per hand. Most (67%) use a wrist entry point; the rest enter via the metacarpal heads. Many (58%) inject into the subdermal plane (superficial dorsal lamina), while 42% inject subfascially (below the superficial dorsal fascia, into the intermediate dorsal lamina).
The anterior abdominal wall was defined as the area between the rectus abdominis muscles and above a horizontal line between the two anterior superior iliac spines, up to the costal margin (Table 11). All Experts first identify the areas with skin laxity and crepiness that require biostimulation before placing fillers subdermally. Most Experts use cannulas to inject 1 to 1.5 cc of CaHA per 100 cm2. Most Experts use diluted CaHA on severe areas and feather more diluted (> 1:1) CaHA around less-problematic areas. The rest treat only problem areas. Over half use 22-/23-gauge cannulas, whereas 33% use 25-gauge cannulas. Over half of the Experts combine CaHA with MFU-V for their synergistic effects in tightening lax skin on the anterior abdominal wall.
For elbow skin biostimulation and tightening, all Experts inject 1.5 cc of filler subdermally per 100 cm2 of treatment area (Table 12). Nearly all would use 22- to 25-gauge cannulas. Over half of Experts dilute 1:1; the rest use higher dilutions (up to 1:2 depending on the patient’s skin thickness and condition). The Experts agreed that the elbows are treated more frequently than the upper arms in female Asian patients; the effects of upper arm treatments are also often less pronounced and were not discussed further. Moreover, all Experts agreed with the Global Consensus recommendations14 to inject hyperdiluted CaHA (1:2 dilution ratio) subdermally when seeking to significantly increase dermal thickness and elasticity in the upper arms. They also agreed with recommendations to treat the circumferential upper arm with 3 mL of CaHA (using two syringes, diluted 1:2 using lidocaine or saline, for a total volume of 9 mL). The Experts also agreed that smaller areas can be treated using one syringe (1.5 mL of CaHA and 3 mL of diluent), as stated in the previous Consensus, although thicker skin may also be treated with CaHA diluted 1:1.

No consensus was reached for forehead augmentation (data not shown); nevertheless, two Experts would inject undiluted filler into the subgaleal plane with cannulas, regardless of whether prior hydrodissection was performed. Local or regional (e.g., supraorbital) nerve blocks would also be given for patient comfort or tumescent hydrodissection would be performed for forehead contouring (these patients experience only mild pain). When pretreatment anesthesia is not used, pain responses are preserved and can signal vascular injury in this high-risk region. For forehead contouring, Experts may dilute CaHA (1:1) for specific patient needs. At least two entry points are used, and a third, central entry point may be created for deep central forehead access. CaHA dose for the whole forehead varied from less than 0.5 cc (8.33%) to 0.5 to 1cc (25%), 1 to 1.5 cc (33.33%), and more than 1.5 cc (33.33%). Supplementary Figure 2 presents some of the potential aesthetic outcomes in the forehead following CaHA injection.

Discussion
This Consensus was discussed in the context of Asian patients and using the suggestions of the Global Consensus as a framework. Generally, the Experts agreed that MFU-V procedures should precede the cannula injection of diluted CaHA (by cannula) during same-day, single-session treatments for shaping and contouring of the face or nonfacial areas, or for skin biostimulation. While the Experts arrived at several areas of agreement, they also differed depending on their access to tools and products and the nature of their patients’ ethnicity-specific preferences and requests. In the face, they agreed that CaHA should be placed in the interfascial layer for temple contouring. In the jawline, it should be placed as struts or microboluses in the subcutaneous plane and combined with same-day MFU-V for jawline contouring and lifting. For the zygoma, less than 0.5 cc of CaHA should be needle-injected supraperiosteally, but, for the anteromedial cheek, 25-gauge or larger cannulas should be used. Cheek contouring is performed with undiluted CaHA, while cheek biostimulation is performed with 1:1 diluted CaHA. For safety, CaHA should not be injected directly into the infraorbital area. For nonfacial or whole-face biostimulation and contouring, diluted CaHA should be injected subdermally.
Two CaHA fillers were considered in these discussions: CaHA and Radiesse®(+), which contains 0.3% integral lidocaine hydrochloride. CaHA has proven longevity as a dermal filler,17,18 and its high elastic modulus (G’) allows it to resist deformation under pressure while providing more lifting power than other dermal fillers.7,19 CaHA is thus ideal for three-dimensional tissue volumization and contouring. Since FDA approval for Radiesse®(+) was given in 2015, many clinicians have adapted the product to their personal clinical practices for different indications,20–22 including upper arm and abdomen skin tightening23 and correcting signs of aging in the hands,24 nasolabial folds,25 and the prejowl.21
The undiluted, nonlidocaine CaHA formulation is highly viscoelastic,14 which contributes to its ability to function as a liquid implant and deliver the tissue support needed for facial revolumization procedures.26 As the classic formulation lacked a local anesthetic agent, physicians manually mixed it with lidocaine solution to improve patient comfort. However, a rheological study demonstrated that mixing CaHA with 2% lidocaine, using a protocol approved by the FDA in 2009, reduced its complex viscosity and G’ by more than half, producing a filler with less deformation resistance and lifting capacity.27 The newer Radiesse®(+), which is formulated with lidocaine particles alongside filler particles, maintains a similar rheological profile to that of undiluted, classic CaHA. It can therefore be applied for lifting and contouring and to improve patient comfort. Notably, Taiwan-based doctors only have access to CaHA, which they usually dilute minimally with lidocaine, highlighting a significant strategic and technical advantage afforded by using undiluted Radiesse®(+) without further mixing.
Although most Asian patients present in their 30s for aging-related facial contouring, certain indications or situations may prompt earlier presentations, including bimaxillary underdevelopment (presenting in the teenage years or early 20s) or acne scarring (in the early 30s). Injectors must therefore determine if these presentations require resolution through contouring and volumization or skin biostimulation and biostimulation. Moreover, unlike Latin American or Caucasian patients, Asian patients are younger at presentation; have distinct skin concerns; and require different dilutions, doses, and specific techniques (e.g., hydrodissection). Asian patients tend to seek earlier interventions than Caucasians and treatment affordability is a factor for presentation in their early 30s. Many Asian women also request body skin biostimulation procedures for postpartum skin changes. However, as the décolletage or buttocks are not frequently exposed, treatment of these areas may be considered unnecessary and even cost-prohibitive if large surface areas are to be treated.
Some areas require analysis in future consensus discussions, such as the forehead. Forehead augmentation is challenging because of the area’s differential anatomy (e.g., skin thickness). This changes during aging to produce a thinner, superficial musculoaponeurotic system; less soft tissue; and less adipose tissue overlying hard bone.28,29 Five types of forehead shapes, depressions, contours, and slopes have been observed in Korean patients, producing deficiencies that require filler-based volume augmentation. These include foreheads with protruding orbital rims and central depressions, foreheads with a suprabrow triangular-shaped depression, and those with a centralized but horizontal depression.29 Anatomically, the forehead scalp tissue comprises a continuous glide plane overlying bone and is a structureless space in which a subgaleal flap can be created during surgery.30 Within this space, some of our Experts consider filler augmentation to be safest; however, others31 prefer to place filler in postperiosteal or preperiosteal spaces, even though these are more difficult to access and/or inject correctly. Central veins and lateral branches from the temporal vessels also require injectors to proceed with care during forehead contouring to maintain injection safety. The fascial bands in the forehead’s deep central compartment hinder the advancement of instruments and an even distribution of fillers.32 The lack of consensus on CaHA dosage for the whole forehead reflects the diverse severities of forehead deficiencies, which consequently determine the filler quantity needed.
The Experts also noted that Asian patients tend to develop horizontal crease marks in the neck, rather than the characteristic crêpe skin observed in Caucasian patients. Thus, neck biostimulation treatments must be formulated differently for Asian patients. As the aging process simultaneously exacerbates neck skin laxity and deepens horizontal necklines, a multimodality approach addressing both aspects will be most effective. Clinical best practices for whole-neck biostimulation and skin tightening with diluted CaHA were diverse, with some Experts also using cannulas to subcise through thick retinacula cutis to lessen the appearance of neck lines. Notably, mechanical subcision can also induce wound healing and, thus, biostimulation. Simultaneous neckline release and biostimulation is achieved during subcision by inserting cannulas perpendicularly through a neckline and depositing hyperdiluted CaHA as a biostimulatory wash during cannula withdrawal. New injectors will know that, when done correctly, the cannula should not encounter any resistance if it is in the subcutaneous plane. Injectors must also note that, given its biostimulatory properties, the main treatment objective of diluted CaHA is to improve neck skin quality and address skin laxity, rather than to correct the appearance of necklines. Such corrections can be successfully achieved through the superficial injection of HA fillers directly into the horizontal necklines at the immediate subdermal plane. However, there is a significant risk of adverse events, such as the Tyndall effect and lumpiness, if an inappropriate HA filler is selected, due to thin skin and lack of adipose tissue in the anterior neck. An ideal choice would be a cohesive polydensified matrix HA (CPM-HA) filler, such as Belotero® Balance (Merz Pharma GmbH & Co. KGaA), which has unique rheological properties of low elastic modulus, low viscous modulus, and high tan delta.33–35 Significant improvement in wrinkle intensity was observed two weeks after CPM-HA injection in patients with horizontal neck wrinkles.35 This improvement persisted with statistical significance throughout the study’s 40-week follow-up and led to excellent levels of physician and patient satisfaction. This success could have been a result of the homogeneous distribution characteristics of CPM-HA when placed intradermally, which prevents the development of surface irregularities and the Tyndall effect.
Veins in the hands of older patients can be fragile and easily damaged by cannulas. Several publications,36–38 have recommended placing cannulas above the superficial fascia in the subdermal plane collagen and elastin fibres to avoid compromising tendons and veins located beneath. However, some Experts are comfortable with placing cannulas into the intermediate lamina to aid delivery of filler particles around veins and to camouflage them without causing danger. Disagreement on the precise locations of tissue structures persists, and though there is evidence to support injecting into subdermal planes (dorsal superficial lamina),37 there is also evidence suggesting that the dermis and superficial fascia adhere tightly.39 In such aged hands, cannulas may be mistaken as situated subdermally when they are actually situated subfascially in the dorsal intermediate lamina.
Abdominal skin treatments can require as many as four CaHA syringes, which is cost-prohibitive for many Asian patients. Some Experts therefore target the more severely affected areas with only two syringes. Others concentrate filler in problem areas and dilute fillers in a tapered and feathered fashion for tissue regeneration in the periphery of problem areas. Using a crosshatched filler-placement pattern can also deliver more filler particles to a specific area.
There are wide variations in the treatment intervals used by different physicians. Some may impose a two- to three-month interval to improve patient compliance, a four- to six-month interval for CaHA tissue integration and neocollagenesis, a one-month interval for increased treatment frequency and more rapid improvements, or a six-month interval for routine maintenance. In fact, extended intervals allow for the development and observation of treatment effects prior to retreatment, while shorter intervals are used mostly by the more proactive clinicians.
With respect to treatment sequence when combining with other modalities, anecdotal evidence suggests that pretreatment with CaHA followed by energy-based devices improves outcomes, as CaHA stimulates tissue remodeling, which enhances the effects of energy-based devices. Many physicians are concerned about filler deformation if MFU-V is performed over areas that have been injected with CaHA. It has been shown that delivery of MFU-V energy immediately after CaHA injection does not alter filler appearance, increase inflammation, or induce product migration, but can even enhance the density and quality of collagen and elastin fibers.40 For both CaHA and MFU-V to be used in the same clinic visit, CaHA injection should be performed first to prevent alteration of tissue planes by the filler that will affect subsequent MFU-V treatment, as well as the potential risk of contamination and infection from nonsterile manipulation of injection entry sites. Individual physician and patient preferences also influence the time at which each modality is used in combination strategies. While many physicians perform same-day procedures to enhance tissue regeneration, those who do different-day procedures wish to allow MFU-V–induced swelling to subside, observe the outcomes of MFU-V before enhancement with CaHA, or to spread out treatment costs. Patients with multiple indications wishing to see immediate results may undergo CaHA injections before returning for MFU-V. In contrast, patients who prefer to begin with a noninvasive treatment may request MFU-V before CaHA injections.
Conclusion
Overall, these discussions highlighted many areas of agreement. On the general usage of CaHA, patients seeking aging-related face contouring are in their early-30s and those seeking biostimulation are between 30 and 50 years of age. On specific CaHA use, dilution is not a critical consideration and should not be confused with dosage, MFU-V should precede CaHA injections in same-day single-session treatments, and 25-gauge cannulas are used where possible. We note that there were also some disagreements as a consequence of the diverse facial morphotypes and desired aesthetic outcomes between Asian ethnicities even within a single Asian country.41 For example, longer faces are more preferred by males in Singapore and Korea than males in Malaysia, while ethnic Chinese in Hong Kong and Taiwan present with euryproscopic faces but seek leptoproscopic face shapes. Shorter faces are more sought after by Malaysian females than other Asian women, while arched brows are preferred by Singaporean, Taiwanese and Malaysian women but not by Thai and Korean females. This disparity underscores the need for customized aesthetic strategies that consider and accommodate the heterogeneous Asian anatomies, ethnicities, attitudes, cultural preferences, and aesthetic ideals of patients across Asia. Disagreements observed during our consensus voting were due to our Experts’ experiences with these differences and to their adaptations to product availability within their geographies as well as their level of expertise with an intervention. Establishing consensus statements to educate new injectors on the most critical aspects of Asian patient treatment considerations, efficacy, and safety is therefore crucial. Taken together, we hope that our areas of consensus or disagreements and our patient case results provide strategic guidance on the use of classic, diluted CaHA for biostimulation or undiluted Radiesse®(+) for lifting and contouring. It is hoped that this knowledge will enable new injectors to master the nuances of CaHA delivery for consistent and successful patient outcomes.
References
- American Society of Plastic Surgeons. 2018 Plastic Surgery Statistics Report. Available at: https://www.plasticsurgery.org/documents/News/Statistics/2018/plastic-surgery-statistics-full-report-2018.pdf. Published 2019. Accessed March 6, 2020.
- Jacovella PF. Use of calcium hydroxylapatite (Radiesse) for facial augmentation. Clin Interv Ageing. 2008;3(1):161–174.
- Montes JR, Wilson AJ, Chang BL, Percec I. Technical Considerations for filler and neuromodulator refinements. Plast Reconstr Surg Glob Open. 2016;4(12 Suppl Anatomy and Safety in Cosmetic Medicine: Cosmetic Bootcamp):e1178.
- Schachter D, Bertucci V, Solish N. Calcium hydroxylapatite with integral lidocaine provides improved pain control for the correction of nasolabial folds. J Drugs Dermatol. 2016 Aug 1;15(8):1005–1010.
- Ahn MS. Calcium hydroxylapatite: Radiesse. Facial Plast Surg Clin North Am. 2007;15(1):85–90.
- Baspeyras M, Dallara J, Cartier H, et al. Restoring jawline contour with calcium hydroxylapatite: a prospective, observational study. J Cosmet Dermatol. 2017;16(3):342–347.
- Loghem JV, Yutskovskaya YA, Werschler WP. Calcium hydroxylapatite: over a decade of clinical experience. J Clin Aesthet Dermatol. 2015;8(1):38–49.
- Friedmann DP. Calcium hydroxylapatite (Radiesse®). In: Goldberg DJ (ed). Dermal Fillers. Vol. 4. Basel, Switzerland: Karger; 2018: 47–80.
- Juhász MLW, Marmur ES. Examining the efficacy of calcium hydroxylapatite filler with integral lidocaine in correcting volume loss of the jawline—a pilot study. Dermatol Surg. 2018;44(8):1084–1093.
- Meland M, Groppi C, Lorenc Z. Rheological properties of calcium hydroxylapatite with integral lidocaine. J Drugs Dermatol. 2016;15(9): 1107–1110.
- Chao YY, Kim JW, Kim J, et al. Hyperdilution of CaHA fillers for the improvement of age and hereditary volume deficits in East Asian patients. Clin Cosmet Investig Dermatol. 2018;11:357–363.
- Juhász MLW, Levin MK, Marmur ES. Pilot study examining the safety and efficacy of calcium hydroxylapatite filler with integral lidocaine over a 12-month period to correct temporal fossa volume loss. Dermatol Surg. 2018;44(1):93–100.
- de Almeida AT, Figueredo V, da Cunha ALG, et al. Consensus recommendations for the use of hyperdiluted calcium hydroxyapatite (Radiesse) as a face and body biostimulatory agent. Plast Reconstr Surg Glob Open. 2019;7(3):e2160.
- Goldie K, Peeters W, Alghoul M et al. Global gonsensus guidelines for the injection of diluted and hyperdiluted calcium hydroxylapatite for skin tightening. Dermatol Surg. 2018;44 Suppl 1:S32–S41.
- Fabi SG, Burgess C, Carruthers A et al. Consensus recommendations for combined aesthetic interventions using botulinum toxin, fillers, and microfocused ultrasound in the neck, décolletage, hands, and other areas of the body. Dermatol Surg. 2016;42(10):1199–1208
- Chao YYY, Chhabra C, Corduff N et al. Pan-Asian consensus—key recommendations for adapting the World Congress of Dermatology consensus on combination treatment with injectable fillers, toxins, and ultrasound devices in Asian patients. J Clin Aesthet Dermatol. 2017;10(8):16–27.
- Goldman MP, Moradi A, Gold MH, et al. Calcium hydroxylapatite dermal Filler for treatment of dorsal hand volume loss: results from a 12-month, multicenter, randomized, blinded trial. Dermatol Surg. 2018;44(1):75–83.
- Bass LS, Smith S, Busso M, McClaren M. Calcium hydroxylapatite (Radiesse) for treatment of nasolabial folds: long-term safety and efficacy results. Aesthet Surg J. 2010;30(2):235–238.
- Sundaram H, Voigts B, Beer K, Meland M. Comparison of the rheological properties of viscosity and elasticity in two categories of soft tissue fillers: calcium hydroxylapatite and hyaluronic acid. Dermatol Surg. 2010;36(Suppl 3):1859–1865.
- Casabona G. Combined use of microfocused ultrasound and a calcium hydroxylapatite dermal filler for treating atrophic acne scars: a pilot study. J Cosmet Laser Ther. 2018;20(5):301–306.
- Muti GF. Open-label, post-marketing study to evaluate the performance and safety of calcium hydroxylapatite with integral lidocaine to correct facial volume loss. J Drugs Dermatol. 2019;18(1):86–91.
- Radiesse® (+) Lidocaine Injectable Implant. Instructions for Use. Available at: https://www.radiesse.com/wp-content/uploads/EM00788-02.pdf. Accessed June 19, 2019.
- Lapatina NG, Pavlenko T. Diluted calcium hydroxylapatite for skin tightening of the upper arms and abdomen. J Drugs Dermatol. 2017;16(9):900–906.
- Gubanova EI, Starovatova PA. A prospective, comparative, evaluator-blind clinical study investigating efficacy and safety of two injection techniques with Radiesse(®) for the correction of skin changes in Ageing hands. J Cutan Aesthet Surg. 2015;8(3):147–152.
- Beer KR. Safety and effectiveness of injection of calcium hydroxylapatite via blunt cannula compared to injection by needle for correction of nasolabial folds. J Cosmet Dermatol. 2014;13(4):288–296.
- Lorenc ZP, Bass LM, Fitzgerald R, et al. Physiochemical characteristics of calcium hydroxylapatite (CaHA). Aesthet Surg J. 2018;38(suppl_1):S8–S12.
- Meland M, Groppi C, Lorenc Z. Rheological properties of calcium hydroxylapatite with integral lidocaine. J Drugs Dermatol. 2016;15(9):1107–1110.
- Kang HG, Youn KH, Kim IB, Nam YS. Bilayered structure of the superficial facial fascia. Aesthet Surg J. 2017;37(6):627–636.
- Kim J. Novel forehead augmentation strategy: forehead depression categorization and calcium-hydroxyapatite filler delivery after tumescent injection. Plast Reconstr Surg Glob Open. 2018;6(9):e1858.
- Mendelson BC. Facelift anatomy, SMAS retaining ligaments and facial spaces. In: Aston SJ, Steinbrech DS, Walden JL (eds). Aesthetic Plastic Surgery. Philadelphia, PA: Saunders Elsevier; 2009: 53–72.
- Lee W, Yoon J, Koh I, et al. Clinical application of a new hyaluronic acid filler based on its rheological properties and the anatomical site of injection. Biomedical Dermatology. 2018;2(1).
- Chao YYY. Saline hydrodissection: a novel technique for the iinjection of calcium hydroxylapatite fillers in the forehead. Dermatol Surg. 2018;44(1):133–136.
- Kablik J, Monheit GD, Yu L, et al. Comparative physical properties of hyaluronic acid dermal fillers. Dermatol Surg. 2009;35(Suppl 1):302–312.
- Santoro S, Russo L, Argenzio V, et al. Rheological properties of cross-linked hyaluronic acid dermal fillers. J Appl Biomater Biomech. 2011;9(2):127–136.
- Tseng F, Yu H. Treatment of horizontal neck wrinkles with hyaluronic acid filler: a retrospective case series. Plast Reconstr Surg Glob Open. 2019;7(8):e2366.
- Rivkin AZ. Volume correction in the ageing hand: role of dermal fillers. Clin Cosmet Investig Dermatol. 2016;9:225–232.
- Frank K, Koban K, Targosinski S, et al. The anatomy behind adverse events in hand volumizing procedures: retrospective evaluations of 11 years of experience. Plast Reconstr Surg. 2018;141(5):650e–662e.
- Kühne U, Imhof M. Treatment of the ageing hand with dermal fillers. J Cutan Aesthet Surg. 2012;5(3):163–169.
- Humzah D. Dorsal hand anatomy: Age-related changes, fat planes and vascular considerations. J Aesthetic Nursing. 2013;2(1):1–4.
- Casabona G, Michalany N. Microfocused ultrasound with visualisation and fillers for increased neocollagenesis: clinical and histological evaluation. Dermatol Surg. 2014;40(Suppl 12): S194–S198.
- Corduff N, Chao YY, Lam SC, et al. A new simplified visual assessment tool describing facial morphotypes observed and desired in Asian populations. J Clin Aesthet Dermatol. 2020;13(4):23–34.