 J Clin Aesthet Dermatol. 2022;15(9):40–44.
J Clin Aesthet Dermatol. 2022;15(9):40–44.
by Howyda Ebrahim, MD; Amany Nassar, MD; Mariam Mohammed Mousa, MSc; and Elsayed Khater, MD
Drs. Ebrahim, Nassar and Khater are with the Faculty of Medicine at Zagazig University in Zagazig, Egypt. Dr. Mousa is with the Faculty of Medicine at Omar Al-Mukhtar University in Al Bayda, Libya. Dr. Khater is an assistant professor of dermatology in Faculty of Medicine at Zagazig University in Egypt.
ABSTRACT: Background. The current treatments of Facial hyperhidrosis (FH) are often limited and are associated with many adverse effects.
Objective. The objective was to study the efficacy and safety of botulinum toxin-A delivery by microneedling versus its intradermal injection in the treatment of FH. Forty-two patients with FH were subjected to microneedling (Mn) followed by topical application of BTX-A on one side of the face and intra-dermal injection of BTX-A on the other side. Two sessions were performed at two week intervals. The assessment tools were Hyperhidrosis Disease Severity Scale (HDSS), the Dermatology Life Quality Index (DLQI), and patient satisfaction.
Results. A score of one of HDSS was achieved in 85.7 percent of patients on the intradermally injected side versus 83.3 percent on the microneedling side (P=0.76%). Most of the patients on the injection side responded with the first session while the microneedling side responded with the second one (P<0.001). The DLQI was highly significant on both sides post-treatment (P<0.001). The side effects were mild in the form of pain on the intradermally injected sides, and mild transient erythema on the microneedling side. The microneedling side showed higher patient satisfaction compared to the intradermally injected side.
Conclusion. Both techniques were safe and effective in controlling the FH. Microneedling delivery of BTX-A was less painful and had higher patient satisfaction.
Keywords. Botulinum toxin Type-A, Facial hyperhidrosis, Hyperhidrosis Disease Severity Scale, Microneedling, Intradermal injection
Hyperhidrosis (HH) is characterized by excessive sweating that exceeds the amount necessary to meet the body’s thermal regulation. Hyperhidrosis often interferes with daily activities and is associated with low self-esteem. Hyperhidrosis is classified into primary or secondary. The primary type has unknown etiology and is characterized by bilateral and symmetrical distribution. Secondary HH may be caused by endocrinal, neurological diseases, infections, or malignancy. The focal type can affect the face, axillae, hands, or feet.1-3 Treatments of HH are often limited. Topical antiperspirants need frequent reapplication, are associated with limited effect, and are intolerable.4-7 Comparatively, the surgical treatments are expensive, require downtime, and are often associated with complications and high recurrence rates.8,9 BTX-A was approved for the treatment of axillary HH. In this study, we tried to use it as an off-label indication as a therapy for FH.10,12 Microneedling (Mn) has been used as therapeutic and also drug delivery.12-13 This study aimed to determine the efficacy of Mn delivery of BTX-A compared to its intradermal injection for the treatment of FH to find out the ideal technique which can provide successful results and a less painful method of drug delivery.
Methods
Study design. A comparative, prospective, randomized split-face study was conducted on 42 patients of both male and female participants with nearly symmetrical hyperhidrosis on both sides of the face. The study was carried out at the Dermatology Department of Zagazig University Hospital in the period from March 2021 to November 2021 after approval of the ethical committee (No; 6809). Informed consent was obtained from all patients. Inclusion criteria for patients’ selection included: relatively bilateral and symmetrical, primary focal HH involving the face, interferes with daily activities, the sweating absent during sleep, and excessive during the last six months. Exclusion criteria were: pregnancy, breastfeeding or menopausal women, patients with diabetes, other medical conditions or endocrinal diseases (causes of secondary FH), patients who received any topical or systemic treatment for FH during the last three months, hypersensitivity to cow’s milk protein, human albumin or iodine were excluded from the study. All participants were subjected to full history and general and dermatological examination.
Treatment protocol. Iodine starch test was performed before each session and two weeks after. The face was cleansed by alcohol and cotton soaked with iodine was applied to the skin. After drying, starch flour was sprinkled on the face. Then, standardized photographs were taken, and the patients were instructed to wash their faces. Each patient received an intradermal BTX-A injection on one side and microneedling on the other side followed by an application of BTX-A.
Intradermal injected side. The face was cleaned with an alcohol solution, and a numbing cream (EMLA, AstraZeneca, Luton, UK) was applied and washed off after 40 minutes before the session. On one side of the face, 1mL of the diluted BTX-A 100 u vial (Botox, Allergan, Germany) was reconstituted by 5ml saline (to yield a concentration of 20U/1mL) was injected intradermally forming bleb or wheal-like. The injection was 1cm apart with an injection of 0.1mL of the insulin syringe (1mL, 30G) injected at each point. The injection was distributed across the forehead 1cm above the supraorbital ridge up to the hairline. The areas that should be avoided were from the nasolabial folds down to the mandible on both sides of the face to avoid an asymmetrical smile. Regarding the upper lip; the area was divided into two halves, three points in each half were injected at 0.5cm between each point, 0.5cm above the lip, and 0.5 m from the philtrum. The total injected dose was 20u/mL.
Microneedling side. On the other side of the face, the microneedling device (Dermapen, Bomtech Electronics, Korea) had a head supplied by 36-needles applied to the treated areas of the face. It was gently moved across the treatment area to create many, tiny, micro-channels. The microneedling depth was adjusted according to the treated area; 0.5mm in diameter in the forehead area and nose, 2mm in the checks, and 1.5mm in the chin area. Three passes were performed in three directions (transverse, vertical, and diagonal) over the area with FH. After reaching the endpoint (pinpoint bleeding), the bleeding was cleaned from the skin surface using saline-soaked gauzes. Then, the same dose of BTX-A used in the Id injection side was dropped directly onto the skin by a 1mL, 30G insulin syringe. The face was left until drying. On both sides, 1mL of diluted BTX-A (100u diluted by 5ml saline) was used for one or two sessions two weeks apart. All patients were reviewed after two weeks, and supplementary points are administered to the areas with continued sweating after performing the iodine starch test. They were also asked to complete a questionnaire for subjective ratings of sweating and their satisfaction with the treatment.
Follow-up. Follow-up was done for six months to check the durability of BTX-A and for the appearance of any side effects.
Clinical Assessment. -HDSS disease-specific diagnostic tool provides a qualitative measure of the severity of the patient’s condition. HDSS score of one or two indicates mild or moderate HH and a score of three or four indicates severe HH. Evaluation of HDSS post-treatment can help to assess the treatment efficacy; when the HDSS was decreased by one point, this means a reduction of 50 percent in sweat intensity (partial response) while the reduction by two points indicates an 80 percent decrease in the intensity of hyperhidrosis (excellent response) and zero scores (no response) means that there are no changes.
Side effects. Any other adverse effects such as pain, edema, or ecchymosis were recorded.
Follow-up. The patients were followed up for six months. The effect lasted for four months in 57.1 percent of the patients and up to five months in 42.9 percent of the patients.
Statistical analysis. Statistical analysis was performed using SPSS version 27.0 (IBM, 2020) (SPSS Inc., Chicago, IL, USA). Chi-square test (χ2), Mc-Nemar test, Independent T-test, and Paired sample T-test were used when appropriate. P values less than 0.05 were considered statistically significant.
Results
A total of 42 patients (18 males and 24 females, with a mean age of 28.31±13.96) with FH participated in this study. Patients’ demographic and clinical data are presented in (Table 1). The baseline HDSS score of both sides of the patient’s face revealed no significant differences. After the treatment, there was a highly significant decrease in sweat production revealed by HDSS (p<0.001) (Figures 1 and 2) (Table 2).
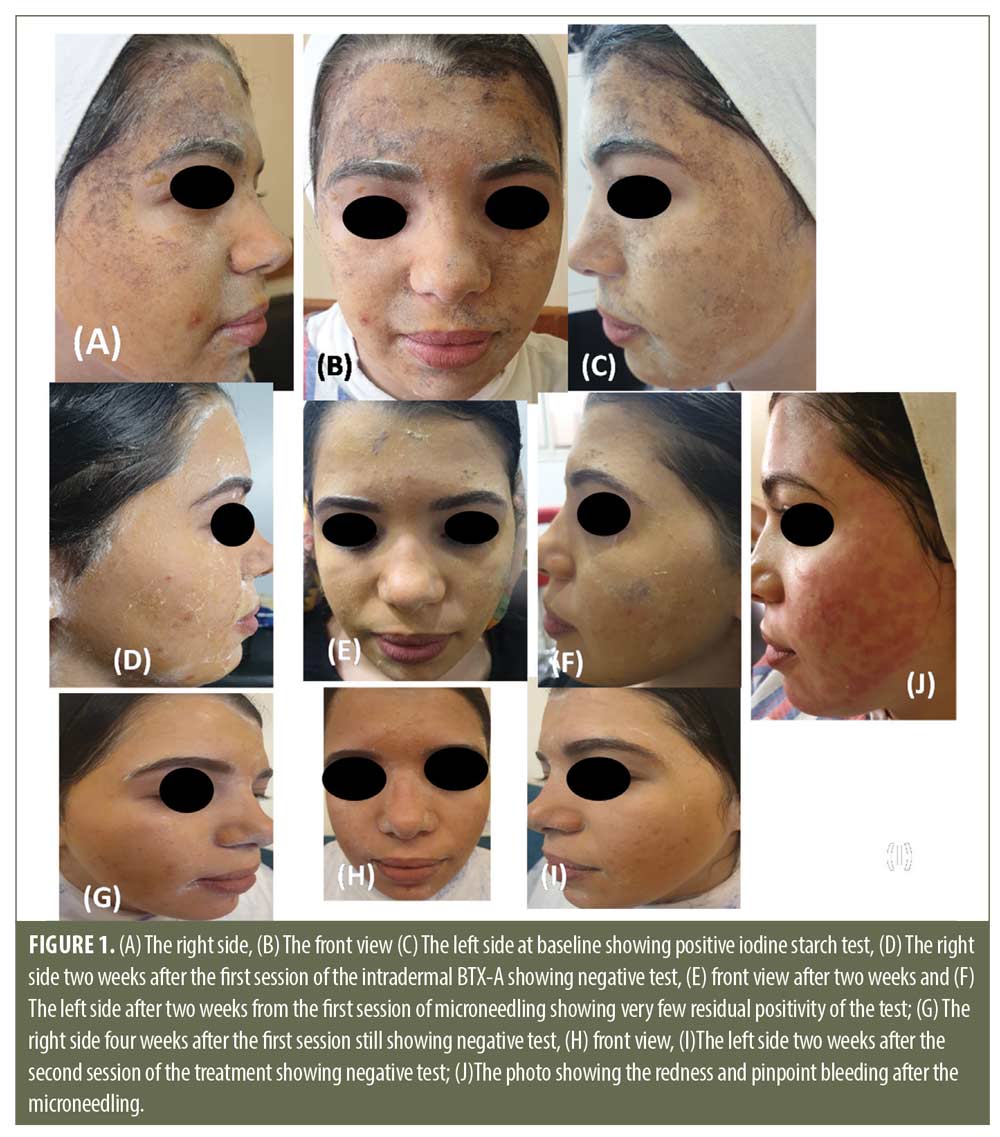
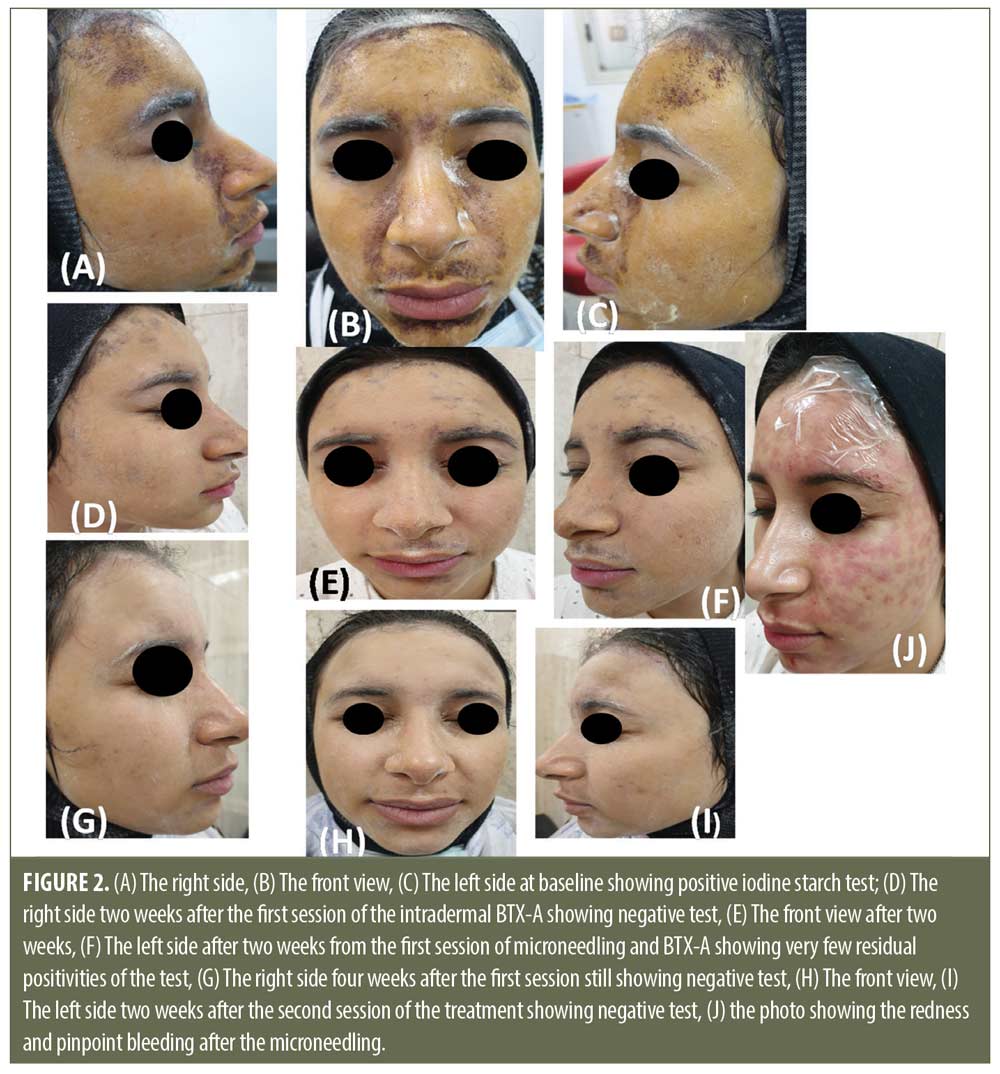

Two weeks after the 1st session. The intradermally injected side. There was a statistically significant decrease in HDSS score (61.9% of the patients achieved a score of 1 and 38.1% achieved a score of 2) (p<0.001) (Table 2).
The microneedling side. On this side, all of the patients achieved a score of two.
Two weeks after the 2nd session. The intradermally injected side. This side showed a significant decrease in HDSS; 85.7 percent of patients achieved a score of 1 and 14.3 percent achieved a score of 2 (p<0.001) (Table 2).
The microneedling side. On this side, 83.3 percent of the patients achieved a score of 1, and 16.7 percent of patients achieved a score of 2.
Three months after 2nd session. Three months after the last session, 78.6 percent of patients still had a score of 1 on the injected side compared to 76, 2 percent on the microneedling side (p=0.79). Patients’ satisfaction was significantly higher on the microneedling side compared to the other side (p<0.03) (Table 3). Regarding the adverse effects, there was a significant increase in the frequency of pain; the pain score was higher on the injected side compared to the microneedling side (p<0.001). Mild erythema and slight edema were noted on the microneedling side (Table 3).
Discussion
Facial hyperhidrosis (FH) has a negative effect on the person’s quality of life. It poses a therapeutic challenge for the patients and also the physicians. The current treatments are not satisfying for most of the patients.16 Botulinum toxin type A (BTX-A) appears the most effective therapy used for the treatment of focal HH (axillary, palmar, and plantar type). However, its intradermal injection is very painful.17 A literature review revealed that using a microneedling delivery of BTX-A for the treatment of FH has never been published. This study aimed to minimize the area of BTX-A diffusion as well as the pain during injections. In this study, DLQI and HDSS were used as primary end-points. After the treatment, the overall improvement was 100 percent on both sides. HDSS score decreased in 61.6 percent of patients after the 1st session on the intradermally injected side and in 85.7 percent of the patients after the second session. On the microneedling side, HDSS decreased after the second session in 83.3 percent of the patients (p<0.001). Both techniques were effective and produced dramatic improvements in patients’ quality of life; as revealed by a decline in DLQI, it decreased to1.3±0.3 on the injected side versus 1.7±0.2 on the microneedling side with no significant difference between both sides. However, there was a significant difference in the number of sessions; most of the patients responded after one session on the injected side, and after two sessions on the microneedling side. The patients judged their satisfaction as very satisfied on 81 percent of patients on the microneedling side versus 59.5 percent on the intradermally injected side. Intradermal BTX-A means using much diluted BTX-A to induce skin rejuvenation, shrink pores, and reduce sebum and sweating secretion.18
Intradermal injected BTX-A targets mainly the skin while the traditional type targets the muscles which may lead to facial asymmetry.19 Therefore, in this study, the rationale for using the intradermal injection of the diluted toxin was that it would have less effect on the muscle which is an important factor during the treatment of frontal hyperhidrosis. However, the intradermal injection requires an experienced physician to minimize the potential risk of diffusion during the injection. So, microneedling delivery is more easily applied even on most areas of the face, and it can provide a less painful technique compared to the injection. Microneedling was used either alone or combined with other therapeutic modalities in the treatment of different dermatologic diseases.12 It enabled BTX-A delivery into the epidermis without affection of the underlying muscles via the open channels which diffused into the superficial muscle fibers without affection of the deeper muscles. Microneedling has many advantages such as it facilitating the BTX-A to reach the exact site, being easily applied, safer, and less painful.13 Intradermal BTX-A has been previously approved for the treatment of axillary hyperhidrosis.16 Trindade et al20 used the intradermal injection of BTX-A in the treatment of twenty patients with craniofacial hyperhidrosis (CFH). The results revealed a 100 percent success rate in all patients. Side effects included were pain during injection and transient inhibition of frontalis muscles. Another study also used the intradermal injection of BTX-A for the treatment of 10 patients with frontal hyperhidrosis; eight of them reported that the treatment was very effective. The treatment was tolerable but the patients suffered from pain during injections and partial loss of the corrugators’ function.21 The authors demonstrated that BTX-A was an effective and safe treatment for FH. However, the intradermal injection of BTX-A was not easily applied to the whole face, which may lead to facial asymmetry, and in addition, it was very painful.21 Karlqvist et al22 treated 38 patients who had CFH by intradermal BTX-B. After treatment, the DLQI scores and sweat were reduced. Most of the patients’ were satisfied (87%) with the results. A side effect was forehead stiffness. Philip et al23 performed a randomized controlled study on eight postmenopausal women with CFH using BTX-A. Post-treatment DLQI score showed 90 percent improvement in all of the patients treated with BTX-type A.
In the current study, most of the patients achieved a score of one (unnoticeable sweating) after one session. Using the superficial injection of BTX-A was associated with better outcomes and fewer adverse effects. Despite the microneedling side consuming one more session in most of the patients, it was painless and had greater patient satisfaction. BTX-A represents an effective and safe treatment option for FH even in the middle and lower parts of the face when a special injection technique is used. In the present study, no serious side effects were noted except mild erythema, subtle edema, and pain during the session were the most common complaint; on the injected side, all of the patients (100%) suffered from moderate pain while on the microneedlig side, only (33.3%) of patients felt discomfort. Both methods were safe and effective in controlling the extreme FH compared to topical treatments, systemic drugs, or invasive surgical techniques. Larger scale studies using comparable outcome measures are recommended to optimize patient outcomes. Using microneedling delivery for BTX-A remains an area that requires further research.
Conclusion
Both intradermal injections of diluted BTX-A or its microneedling delivery could be the first therapeutic option for FH owing to their safety and efficacy particularly if the patient was not satisfied with the topical treatment. Microneedling delivery of BTX-A was less painful and had greater patient satisfaction.
References
- Hashmonai M, Cameron AE, Connery CP, et al. The etiology of primary hyperhidrosis: a systematic review. Clinical Autonomic Research2017;6:379–383.
- Hoorens I, Ongenae K. Primary focal hyperhidrosis: current treatment options and a step-by-step approach. Journal of the European Academy of Dermatology and Venereology. 2012;1:1–8.
- Glaser DA, Hebert AA, Pariser DM, et al. Facial hyperhidrosis: best practice recommendations and special considerations. Cutis. 2007;79:29–32.
- Lear W, Kessler E, Solish N, et al. An epidemiologic study of hyperhidrosis. Dermatol Surg. 2007;33: S69–75.
- Hasimoto EN, Cataneo DC, Dos Reis TA, et al. Hyperhidrosis: prevalence and impact on quality of life. J Bras Pneumol. 2018;44:
292–298. - Hongbo Y, Thomas CL, Harrison MA, et al. Translating the science of quality of life into practice: What do dermatology life quality index scores mean? J Invest Dermatol. 2005; 125: 659–664.
- Hamm H. Impact of hyperhidrosis on quality of life and its assessment. Dermatol Clin. 2014;32:467–476.
- Grabell DA, Hebert AA. Current and emerging medical therapies for primary hyperhidrosis. Dermatology and therapy.2017;1:25–36.
- Murray CA, Cohen JL, Solish N. Treatment of focal hyperhidrosis. J Cutan Med Surg 2007;11:67–77.
- Shetty MK. Guidelines on the use of botulinum toxin Type A. Indian J Dermatol Venereol Leprol. 2008;74:13–22.
- Heckmann M, Breit S, Ceballos BA et al. Side-controlled intradermal injection of botulinum toxin A in recalcitrant axillary hyperhidrosis. J Am Acad Dermatol. 1999; 41: 987–990.
- Tejashree W, Gautam S, Sunil KD, et al. Microneedles: A smart approach and increasing potential for transdermal drug delivery system. Biomedicine & Pharmacotherapy. 2019; 109: 1249–1258
- Bariya SH, Gohel MC, Mehta, TA, et al. Microneedles: Anew emerging transdermal drug delivery system. J Pharm Pharmacol. 2012; 64:11–29.
- Kamudoni P, Mueller B, Halford J, et al. The impact of hyperhidrosis on patients’ daily life and quality of life: a qualitative investigation. Health and quality of life outcomes.2017;1:1–10.
- Doha O, Mustafa S, Alperen S, et al. Botulinum Toxin Versus Placebo: A Meta-Analysis of Treatment and Quality-of-life Outcomes for Hyperhidrosis. Aesth Plast Surg. 2021; 45:1783–1791.
- Nawrocki S and Cha J. The etiology, diagnosis, and management of hyperhidrosis: A comprehensive review: Etiology and clinical work-up. Journal of the American Academy of Dermatology. 2019; 81:657–666.
- Swartling C, Naver H, Lindberg M. Botulinum A toxin improves life quality in severe primary focal hyperhidrosis. Eur J Neurol. 2001; 8:247–252.
- Shah AR. Use of intradermal botulinum toxin to reduce sebum production and facial pore size. J Drugs Dermatol. 2008;7:847–850.
- Rose AE, Goldberg DJ. Safety and efficacy of intradermal injection of botulinum toxin for the treatment of oily skin. Dermatol Surg. 2013; 39(3 Pt 1):443–448.
- Trindade de Almeida AR, Marques E, de Almeida J, et al. Pilot study comparing the diffusion of two formulations of botulinum toxin type A in patients with forehead hyperhidrosis. Dermatol Surg. 2007;33:37–43.
- Kinkelin I, Hund M, Naumann M. Effective treatment of frontal hyperhidrosis with botulinum toxin A. Br J Dermatol. 2000;143(4):824–827.
- Karlqvist MK, Rosell A, Rystedt K, et al. Botulinum toxin B in the treatment of craniofacial hyperhidrosis. JEADV. 2014; 28: 1313–1317.
- Philip C, Carl S, Alma R. Postmenopausal craniofacial hyperhidrosis treated with botulinum toxin type B. Journal of Dermatology. 2019; 46: 874–878.