Dominique Fausto de Souza, MD, Sector of Dermatology, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil; Lilian Micaelo, MD, Sector of Dermatology, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil; Tullia Cuzzi, MD, PhD, Sector of Pathology, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil; Marcia Ramos-e-Silva, MD, PhD, Sector of Dermatology, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil
Abstract
Plantar fibromatosis, or Ledderhose disease, is a rare hyperproliferative disorder of the plantar aponeurosis. It may occur at any age with the greatest prevalence at middle age and beyond. This disorder is more common in men than woman and it is sometimes associated with other forms of fibromatosis. A 28-year-old Brazilian woman with a six-year history of painless bilateral plantar nodules is described in this article. (J Clin Aesthet Dermatol. 2010;3(9):45–47.)
Plantar fibromatosis, or Ledderhose disease (LD), is a rare hyperproliferative disorder of the plantar aponeurosis first described in 1894 by Dr. Georg Ledderhose.1 Its etiology is unknown. The condition is essentially benign and often associated with Dupuytren’s disease. The patient described in this article is a young woman with bilateral disease, no family history, and no predisposing factors associated with fibromatosis.
CASE REPORT
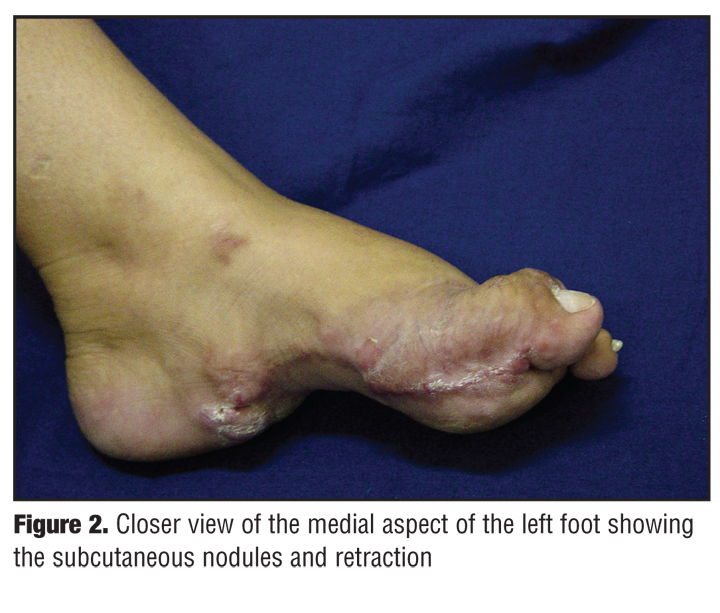
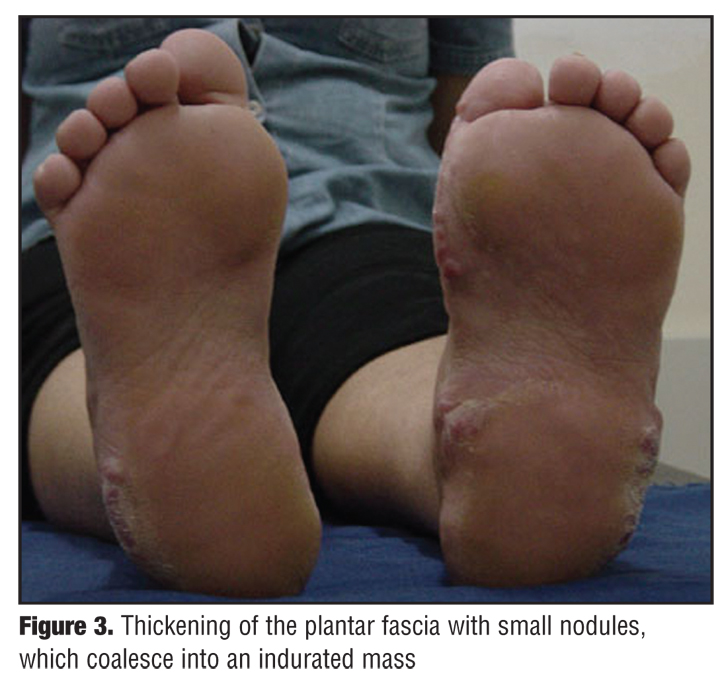
A 28-year-old Brazilian woman presented with a six-year history of painless bilateral plantar nodules. On examination, she had subcutaneous nodules on the lateral aspect of both feet (Figure 1) and on the medial aspect of the left foot (Figure 2). She had thickening of the plantar fascia with small nodules, which coalesced into an indurated mass (Figure 3). The patient also had flexion contracture of the left hallux. Neither Dupuytren’s disease nor knuckle pads were detected. There was no family history of similar nodules. The patient was not taking any medication and was otherwise healthy.
{kind=link}
{kind=link}
{kind=link}
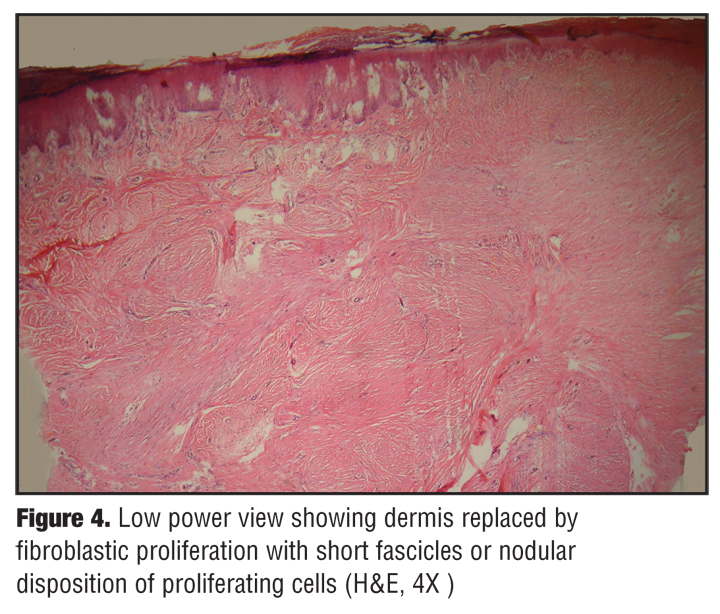
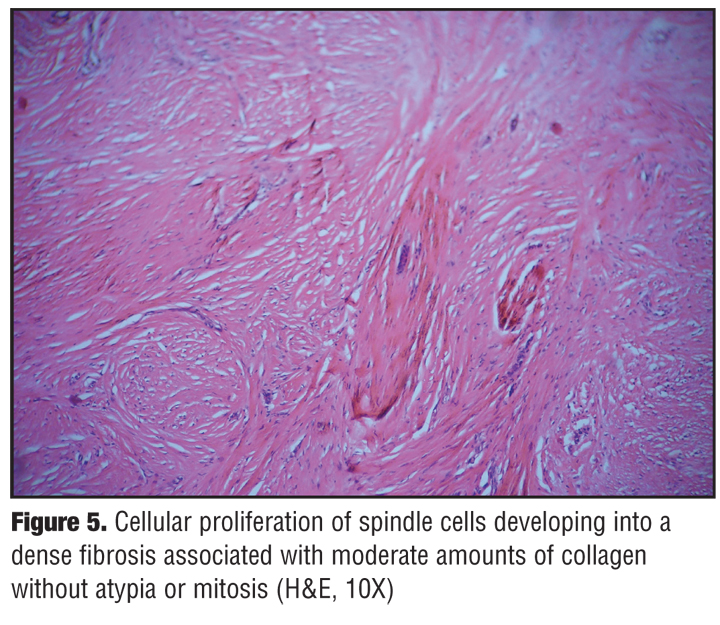
Histological examination of a nodule demonstrated fibroblastic proliferation developing into a dense fibrosis. The nuclei of the fibroblasts were of uniform morphology, elongated, and without atypia or mitosis (Figure 4, Figure 5, and Figure 6). The cells were CD34 negative.
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
Superficial fibromatosis includes plantar fibromatosis (Ledderhose disease), palmar fibromatosis (Dupuytren’s disease), penile fibromatosis (Peyronie’s disease), and knuckle pads. Although its incidence is well described on the hands, it is less commonly seen on the feet.
LD is a relatively rare foot disorder of unknown etiology. Although it is listed as a “rare disease” by the Office of Rare Diseases (ORD) of the National Institutes of Health (NIH), which means that it affects less than 200,000 people in the United State’s population,[2] there are authors who report Ledderhose disease as a relatively common condition, with plantar contracture developing in approximately 25 percent of middle-aged or elderly individuals (1 of every 4 with Dupuytren’s contracture).[3]
It is characterized by local proliferation of abnormal fibrosis tissue in the plantar fascia. The nodules are typically slow growing and most often found in the central and medial portions of the plantar fascia. This tissue is locally aggressive and progressively replaces the normal plantar aponeurosis.[4]
LD may occur at any age with the greatest prevalence at middle age and beyond. This disorder is more common in men than woman and it is sometimes associated with other forms of fibromatosis, such as Dupuytren’s disease in the hand, Peyronie’s disease, or knuckle pads. Only 25 percent of patients have bilateral involvement.[4]
In LD, as in Dupuytren’s contracture, repeated trauma, diabetes, and epilepsy have been reported in association with the development of the lesions.[4–6]
Children may also be affected by this process. Fetsch et al[7] described 56 cases of palmar-plantar fibromatosis in children and preadolescents. A family history was available for 25 patients. Only one patient had concurrent disease involving both feet. Jacob et al[8] proposed the term benign anteromedial plantar nodules of childhood to describe the distinct pediatric form of plantar fibromatosis.
Although in Dupuytren’s disease an autosomal dominant inheritance has been demonstrated, familial cases of plantar fibromatosis are rare.[9] Dartoy et al[10] examined the relatives of seven patients with plantar fibromatosis and did not find any cases. Sammarco et al11 reported one familial case in a series of 18 patients, suggesting that inherited plantar fibromatosis is very rare. Graells Estrada et al[9] reported an additional case of familial plantar fibromatosis.
For reasons unique to the anatomy of the plantar fascia, contracture of the toes is rare.[12,13] A differential diagnosis for the heel pain along the medial arch could be a benign thickening of the plantar fascia associated with plantar fibromatosis.[14]
Nonsurgical treatments of LD include intralesional cortisone injections,15,16 stretching, orthotics, and nonsteroidal antirheumatic drugs and physiotherapy.[16]Nonsurgical treatments should be performed when clinical symptoms occur. Surgical treatment is indicated in cases of persistent pain. The standard procedure includes a partial fasciectomy of the plantar aponeurosis.[16] After partial resection, there is a high recurrence rate with an increased risk of complications and more aggressive ingrowth into anatomical structures.[16,17] Some authors recommend a complete fasciectomy as the primary procedure of choice.[16–18] Postoperative radiotherapy can be used to diminish the chance of recurrence.[19]
Any dermatologist who discovers Garrod’s nodes or knuckle pads should search for early fibromatosis of the palmar and plantar fascia, or at least warn the otherwise unaffected patient that he or she may be susceptible to the development of palmar and plantar fibromatosis and Peyronie’s disease.[20]
References
1. Ledderhose G. Über zerreisungen der plantarfascie. Arch Klin Chir. 1894;48: 853–856.
2. Prevalence and incidence of Ledderhose disease. http://www.wrongdiagnosis.com/l/ledderhose_disease/ prevalence.htm. Accessed on April 19, 2010.
3. Hougeir FG, Mascaro JM. Plantar fibromatosis. http://emedicine.medscape.com/article/1061903-overview. Updated Jun 30, 2009. Accessed on April 19, 2010.
4. Jan Van Der Bauwhede MD. Ledderhose disease: plantar fibromatosis. In: Wheeless’ Textbook of Orthopaedics; 2007.
5. Flatt AE. The Vikings and Baron Dupuytren’s disease. Proc (Bayl Univ Med Cent). 2001;14 (4):378–384.
6. Elhadd TA, Ghosh S, Malik MI, Collier A. Plantar fibromatosis and Dupuytren’s disease: an association to remember in patients with diabetes. Diabet Med. 2007;24(11):1305.
7. Fetsch JF, Laskin WB, Miettinen M. Palmar-plantar fibromatosis in children and preadolescents: a clinicopathologic study of 56 cases with newly recognized demographics and extended follow-up information. Am J Surg Pathol. 2005;29(8):1095–1105.
8. Jacob CI, Kumm RC. Benign anteromedial plantar nodules of the childhood: a distinct form of plantar fibromatosis. Pediatr Dermatol. 2000;17(6):472–474.
9. Graells Estrada J, Garcia Fernández D, Badia Torroella F, Moreno Carazo A. Familial plantar fibromatosis. Clin Exp Dermatol. 2003;28(6):669–670.
10. Dartoy C, Le Nen D, Riot O, Lefevre C, Courtois B. Ledderhose’s disease. Report of 7 cases. J Chir (Paris). 1990;127(11):533–536.
11. Sammarco GJ, Mangone PG. Classification and treatment of plantar fibromatosis. Foot Ankle Int. 2000;21(7):563–569.
12. Donato RR, Morrison WA. Dupuytren’s disease in the feet causing flexion contractures in the toes. J Hand Surg [Br]. 1996;21(3):364–366.
13. Classen DA, Hurst LN. Plantar fibromatosis and bilateral flexion contractures: a review of the literature. Ann Plast Surg. 1992;28(5):475–478.
14. Zgonis T, Jolly GP, Polyzois V, Kanuck DM, Stamatis ED. Plantar fibromatosis. Clin Podiatr Med Surg. 2005;22(1): 11–18.
15. Pentland AP, Anderson TF. Plantar fibromatosis responds to intralesional steroids. J Am Acad Dermatol. 1985; (1 Pt 2):212–214.
16. Beckmann J, Kalteis T, Baer W, Grifka J, Lerch K. Plantar fibromatosis: therapy by total plantar fasciectomy. Zentralb Chir. 2004;129(1):53–57.
17. Wapner KL, Ververeli PA, Moore JH Jr, et al. Plantar fibromatosis: a review of primary and recurrent surgical treatment. Foot Ankle Int. 1995;16(9):548–551.
18. Durr HR, Krodel A, Trouillier H, Lienemann A, Refior HJ. Fibromatosis of the plantar fascia: diagnosis and indications for surgical treatment. Foot Ankle Int. 1999;20(1):13–17.
19. de Bree E, Zoetmulder FA, Keus RB, Peterse HL, van Coevorden F. Incidence and treatment of recurrent plantar fibromatosis by surgery and postoperative radiotherapy. Am J Surg. 2004;187(1):33–38.
20. Connely TJ, Stuart DO. Development of Peyronie’s and Dupuytren’s diseases in an individual after single episodes of trauma: a case report and review of the literature. J Am Acad Dermatol. 1999;41:106–108.