Novie Sroa, MD, Larisa Ravitskiy, MD—The Division of Dermatology, The Ohio State University Medical Center, Columbus, Ohio; Shannon Campbell, DO; Ohio University College of Osteopathic Medicine, Department of Specialty Medicine, O’Bleness Memorial Hospital, Athens, Ohio
Abstract
Mohs micrographic surgery has become the “gold standard” for surgical excision of nonmelanoma skin cancers for maximal preservation of normal tissue. Mohs micrographic surgery entails processing specimens in horizontal frozen sections with immediate examination under a light microscope. This technique offers the examination of lateral and deep margins in the same plane in contrast to wide local excision. Success with Mohs micrographic surgery depends on accurate mapping of the tumor, correct interpretation of the histopathological sections, and appreciation of aggressive tumor characteristics. The most common reason for recurrence of tumor after Mohs micrographic surgery is residual undetected tumor. Because hematoxylin and eosin stains may present difficulties in interpretation, immunohistochemistry techniques are being used to supplement these routine stains. Although immunohistochemistry is not being widely utilized by Mohs micrographic surgery surgeons, the many advantages of immunohistochemistry over routine staining of frozen sections in selected settings is of great value. Herein, the authors review the application of immunohistochemistry in Mohs micrographic surgery for a variety of neoplasms encountered most frequently by Mohs micrographic surgery surgeons. (J Clin Aesthetic Dermatol. 2009;2(7):37–42.)
Mohs micrographic surgery (MMS) has become the “gold standard” for surgical excision of nonmelanoma skin cancers for maximal preservation of normal tissue. MMS entails processing specimens in horizontal frozen sections with immediate examination under a light microscope. This technique offers the examination of lateral and deep margins in the same plane in contrast to wide local excision (WLE). Standard histological examination of excision specimens demonstrates only 0.2 percent of the margins; whereas, MMS examines 100 percent of both deep and peripheral margins.[1]
Success with MMS depends on accurate mapping of the tumor, correct interpretation of the histopathological sections, and appreciation of aggressive tumor characteristics. Because hematoxylin and eosin (H&E) staining may present difficulties in interpretation of frozen sections, rapid immunohistochemistry (IHC) techniques are being used to supplement these routine stains. In a recent survey of 108 laboratories processing MMS surgery specimens, 87 percent used H&E stains to process sections. In this same survey, only 13 laboratories used IHC staining of frozen sections.[2]
Adjunctive use of IHC in H&E frozen sections enhances tissue interpretation and spares resection of additional tissue. The most common reason for recurrence of tumor after MMS is residual undetected tumor. Polyclonal antibodies used in IHC offer greater sensitivity than routine H&E stains. Examination of frozen sections of aggressive cutaneous neoplasms, such as melanoma, has been facilitated by IHC. Advances in IHC have addressed issues of cost and time inefficiency in processing MMS frozen sections. IHC leads to facilitated surgical excision via MMS by reducing variable staining, high background or nonspecific staining, and turn-around time. Specifically, IHC is useful in clearly delineating malignant cells present in dense inflammation, identifying perineural invasion and pagetoid spread in carcinomas.[3–6]
While there are several advantages to utilizing IHC in MMS, there are some drawbacks as well. First, IHC stains were initially developed for permanent sections and not frozen sections. Consequently, there are problems with displacement of soluble antigens on frozen sections. Second, using polyclonal antibodies causes decreased specificity because some antigens identified by polyclonal antibodies may belong to normal tissue. Another concern is the incubation time required for each stain, which has been shortened by using higher antibody titers.[2,3]
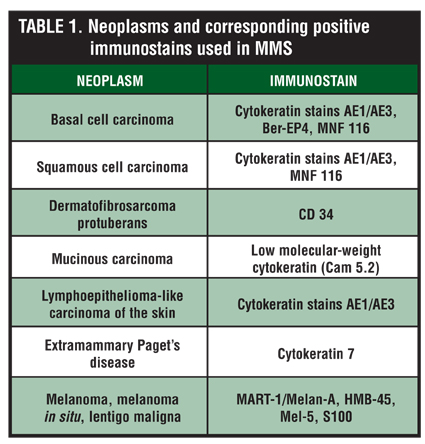
As MMS is increasingly used for high-risk tumors, it is imperative that the dermatology community be familiar with the advances in MMS techniques, especially IHC. Although IHC is not being widely utilized by MMS surgeons, the many advantages of IHC over routine staining of frozen sections in selected settings is of great value. Herein, the authors review the application of IHC in MMS for a variety of neoplasms encountered most frequently by MMS surgeons (Table 1).
{kind=link}
Basal and Squamous Cell Carcinomas
Basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) are the most common cutaneous malignancies. For the purposes of this paper, the authors will refer to both BCC and SCC as nonmelanoma skin cancers (NMSC). The majority of these tumors are managed with superficial ablative techniques and excision, but these have an average of a 10- to 15-percent recurrence rate after five years. MMS has cure rates in the range of 96 to 99 percent. MMS is indicated for high-risk NMSCs, most frequently occurring on the head and neck region of both genders, especially in high-risk anatomical locations, such as periorbital, perinasal, periauricular, and perioral regions.[7–9] These sites, with rich neurovascular supply, warrant maximum tissue preservation. Therefore, differentiation of malignant tissue from benign tissue on histopathology is of utmost importance for preservation of tissue function and cosmesis.
A common tumor phenomenon on BCC frozen sections is folliculocentric basaloid hyperplasia (FBH). It is defined as multifocal basaloid proliferations of uniform cells showing peripheral palisading with or without follicular epithelial involvement. These basaloid aggregates are oriented vertically on horizontal sections and can radiate from normal hair follicles toward skin edges.[7,8] The similarity of histological features between BCC and FBH, especially in locations containing abundant hair follicles, complicates the distinction between BCC variants with follicular differentiation and normal hair follicles. FBH misinterpreted as BCC can compromise tissue preservation in cosmetically sensitive areas if the MMS surgeon excises another layer to achieve tumor-free margins. Subsequent serial sections may provide enough criteria to demonstrate FBH, but will cost the surgeon valuable time and resources.[7–9]
Krunic et al have demonstrated absence or reduction in desmosomes in BCCs via antidesmoglein 33-3D antibody. This monoclonal antibody recognizes cytoplasmic domains of human desmogleins, which are decreased in NMSCs. It serves as a valuable tool in delineating BCC tumor islands from both hair follicles and FBH when morphological criteria are lacking.[9–11]
Although BCC and SCC cells can be easily delineated on frozen sections in most cases, tumor cells of aggressive histopathological type or those that are adjacent to inflammation are difficult to identify. No specific markers exist for either BCC or SCC. However, various reports in the literature describe the use of adjuvant IHC on MMS frozen sections to label cells of epithelial origin versus inflammatory cells. Jimenez et al used anti-cytokeratin 14 and broad-spectrum anti-cytokeratin antibody, AE1/AE3, to more accurately map out tumor cells within dense inflammatory aggregates. The extent of morpheaform BCC tumor cell islands and presence of single-cell perineural invasion is more readily apparent with these antibodies.[7]
Another useful marker, antihuman epithelial antigen (Ber-EP4), detected BCC cells on final MMS margins that were negative on routine staining. MNF 116 is the latest IHC marker reported in the literature for staining aggressive BCCs and SCCs. It has high sensitivity for tumor detection of epithelial cells since it is positive for a number of cytokeratins including 5, 6, 8, 17, and 19. MNF 116, with or without the use of p63 nuclear marker, can aid in identification of poorly differentiated SCC, especially when tumor cells comprise single cells in the dermis.12,13 In their study, Smeets et al demonstrated positive staining with MNF 116 on a slide of morpheaform BCC that was negative by H&E staining. Their conclusion of high sensitivity of adjuvant cytokeratin staining for select cases of aggressive BCCs is supported by another study.[9] Ramnarin et al successfully demonstrated use of MNF 116 and DAKO PL34 for detecting small strands of morpheaform BCC, which otherwise would have been missed on routine stain.[14]
Dermatofibrosarcoma Protuberans
Dermatofibrosarcoma protuberans (DFSP) is the malignant counterpart of dermatofibroma (DF). It is a rare, intermediate-grade, fibrohistiocytic tumor of the dermis with a propensity to recur after local excision. The standard of care has been WLE with margins of 2.5cm or greater.[17] However, the recurrence rates, which are as high as 50 to 75 percent in head and neck cases, have caused increased morbidity. In contrast, the five-year recurrence rate after MMS is in the range of 0 to 7 percent in multiple studies. Marginal recurrence rates range from 0 to 3 percent after five-year follow up.[15–17] MMS is now recommended as first-line treatment for DFSP.
CD34 antibody is most commonly used to aid in the assessment of margins for DFSP. Especially important is the neoplastic cells’ tendency to stain well with CD34 as compared to the normal cells of DF. This stain easily highlights tumor margins that may appear to be negative on routine histological examination.[15–17] A retrospective study of 16 patients with DFSP treated with MMS utilizing CD34 staining demonstrates no recurrence. However, caution has to be maintained due to variable staining patterns since nodular DFSP can be CD34 negative when compared to plaque DFSP.[15,18]
Mucinous Carcinoma
Mucinous carcinoma is a rare cutaneous neoplasm most often occurring on the face, especially eyelids. It is particularly difficult to histologically distinguish mucinous carcinoma from cutaneous metastases of breast, gastrointestinal tract, ovary, prostate, and lung carcinomas. MMS has been used to obtain tumor-free margins with no signs of recurrence in up to five years of follow up. The tumor can be locally destructive with a high recurrence rate of 34 to 43 percent after WLE and occurs in cosmetically sensitive areas requiring optimum tissue preservation.[19–21] Therefore, MMS with adjunctive IHC techniques appears valuable in enhancing the sensitivity of microscopic detection of mucinous carcinoma. The only reported case of mucinous carcinoma treated with MMS and IHC utilized low molecular-weight cytokeratin (Cam 5.2) on MMS frozen sections. This cytokeratin antibody detected residual foci of the tumor that were difficult to identify on routinely stained sections, and it aided in complete tumor removal with no evidence of clinical recurrence at three-year follow up.[22]
Lymphoepithelioma-like Carcinoma of the Skin
Lymphoepithelioma-like carcinoma of the skin (LLCS) histologically resembles nasopharyngeal lymphoepithelioma. On microscopic examination, LLCS presents as atypical polygonal cells with prominent nucleoli arranged in nodules surrounded by dense lymphoplasmacytic infiltrate, complicating clear delineation of tumor cells. LLCS has a poorly differentiated histology, but a relatively good prognosis. However, it has a high recurrence rate from incomplete excision and metastasis to regional lymph nodes.[22–24] Moreover, one case of fatal distant metastasis has also been reported.[23] These characteristics of LLCS make it amenable to excision via MMS. There are six reported case of LLCS successfully treated with MMS with maximum follow up of 20 months without evidence of disease.[25] Jimenez et al have successfully utilized IHC with MMS to treat a case of LLCS. The patient showed no signs of recurrence in 12 months of follow up. LLCS stains with high molecular-weight cytokeratins and epithelial membrane antigen, demonstrating the tumor’s epithelial origin. Hence, rapid immunostaining with AE1/AE3 successfully distinguishes the malignant cells from the neighboring inflammatory cells in their case.[26]
Extramammary Paget’s Disease
Extramammary Paget’s disease is a rare cutaneous adenocarcinoma that occurs as a primary process or as epidermotropic metastases from an underlying contiguous or noncontiguous carcinoma. Because initial diagnosis is often delayed, the tumor quickly metastasizes through dermal lymphatics and as many as 10 percent of patients may have lymph node involvement at presentation.[27–30] In addition to H&E staining, IHC is important to confirm and define tumor margins. Cytokeratin 7 has been the immunostain of choice for evaluating permanent section margins.[31–32] As depicted in Figure 1 , cytokeratin-7 stain was used successfully to delineate an otherwise obscure tumor on an H&E-stained frozen section. In a retrospective review of treatment of extramammary Paget’s disease by O’Connor et al, intraoperative cytokeratin-7 staining was helpful in delineating the disease. Carcinoembryonic antigen was also positive in 2 of the 4 MMS cases in this study.
{kind=link}
Melanoma, Melanoma In situ,Lentigo Maligna
Several stains have been used to identify melanocytes when evaluating melanoma with MMS, including S-100, human melanoma black-45 (HMB-45), Mel-5, and MART-1 (melanoma antigen recognized by T-cells 1 staining) also known as Melan-A.[33] The utilization of stains is guided by the type of melanoma and the stain’s sensitivity and specificity for melanoma. For example, S-100 staining remains the best diagnostic marker in desmoplastic and spindle cell melanoma.[34] Furthermore, Zalla et al found that Melan-A was the most reliable stain for melanoma while HMB-45 appeared to be the least consistent stain.[35]
HMB-45. HMB-45 is a proliferative marker that recognizes glycoprotein 100 in immature melanosomes. Immature melanosomes are found in growing, undeveloped melanocytes, and are characteristic of melanoma. However, immature melanosomes are also found in benign melanocytic lesions, inflammatory skin conditions, skin over vascular structures and near scar tissue, and neonatal skin. While HMB-45 may be specific for melanocytic tumors, it has lacked consistent sensitivity in the detection of melanomas.[35]
Zalla et al found that HMB-45 stained positively in only 85 percent of all melanoma cases and offered a slight advantage of decreased background staining due to HMB-45’s lack of keratinocyte affinity.[35] HMB-45 has been found to be more specific than S-100 for melanocytic lesions but inconsistent with identifying desmoplastic melanomas.[36] In addition, while HMB-45 correctly identifies most melanomas, it has failed to stain isolated areas of in situ and invasive melanocytic proliferations that were recognized by other immunostains.[34]
When comparing frozen sections and H&E permanent sections, Menaker et al reported a concordance of 100-percent sensitivity and 95-percent specificity of HMB-45 staining of melanoma and melanoma in situ (MIS).[37] Similar results have also shown HMB-45 to be useful in paraffin-embedded sections and demonstrated HMB-45’s utility over S-100.[38,39] In addition, Griego and Zitelli reported the effectiveness of HMB-45 for margin analysis in a case of recurrent acral melanoma. In their case, HMB-45 was useful to detect positive margins and became negative as final margins were achieved. However, HMB-45 failed to identify many areas of melanocyte proliferation when MART-1 was positive.[40]
Positive staining for HMB-45 may suggest the presence of malignant melanocytes, but the absence of HMB-45 does not rule out the diagnosis of melanoma as illustrated in a case reported by Albertini et al.[34] While HMB-45 is highly specific, its low sensitivity makes it an unreliable choice as a sole stain to evaluate melanoma margins in MMS.
Mel-5. Mel-5, a murine IgG antibody against melanosomal glycoprotein 75, readily stains for epidermal melanocytes and can be used on both frozen and paraffin-embedded sections. Mel-5 also stains for epidermal components of benign nevi, basal layer epithelial cells containing melanosomes transferred from melanocytes and melanoma. However, Mel-5 does not consistently stain amelanotic melanoma, desmoplastic melanomas, or the dermal component of melanomas. Gross et al reported that epidermally confined lentigo maligna can be reliably excised via MMS using Mel-5 for margin control. Moreover, Mel-5 was found to be superior to S-100 in intensity and specificity with less background interference.[41] However, it is less specific than HMB-45 and can stain positive for nonmelanocytic lesions such as pigmented keratoses, pigmented squamous cell carcinomas, and lichen-planus-like keratoses.35 Overall, Mel-5 appears to be especially valuable for melanomas confined to the epidermis.
Melan-A or MART-1. The MART-1 or the Melan-A antigen has been praised as a vigorous and reliable marker and is able to detect epidermal, junctional and even dermal melanocytes that may be less obvious with HMB-45 or S-100.[34] Melan-A is present in 80 to 100 percent of melanomas and also stains adult melanocytes and nevus cells in the epidermis and dermis.[35]
De Vries et al challenged the superiority of Melan-A over HMB-45. Their studies concluded that Melan-A has a high degree of sensitivity in detecting melanocytes, but a low degree of specificity in differentiating malignant melanocytes from benign melanocytes.[42] Nonetheless, several authors have found MART-1/Melan-A to be a reliable tool for margin analysis.[34,35] In comparison to HMB-45 or S-100, MART-1/Melan-A was found to be more sensitive43 and has been identified as the stain of choice for margin assessment.[33,35] Albertini et al also found Melan-A to be reliably superior when compared to S-100 or HMB-45.[34] Moreover, a Melan-A one-hour protocol developed by Bricca et al demonstrated that Melan-A was reproducibly specific for staining melanoma melanocytes,44 and Hendi et al confirmed that Bricca’s protocol is the most practical and efficient method for melanoma margin analysis in MMS to date.[45] A study performed by Blessing et al demonstrated that Melan-A applied to paraffin-embedded sections stained 97 percent of primary melanomas and 81 to 89 percent of metastatic tumors while HMB-45 stained 90 percent of primary and 75 to 76 percent of metastatic melanomas. In addition, they observed that Melan-A was inferior to S-100 for the staining of spindle cell and desmoplastic melanoma.[36] In summary, Melan-A or MART-1 staining is considered to be the most effective single stain used in the evaluation of melanomas with epidermal and dermal components excluding desmoplastic and spindle cell melanoma types.
S-100. S-100 is the most important historical stain for melanoma. It is a polyclonal antibody to a protein derived from cow brain.[46] The S-100 molecule consists of two subunits—an alpha unit that reacts with axons and melanocytes and a beta unit that reacts with Schwann cells.[36,47,48] S-100 stains almost all benign melanocytic lesions as well as a variety of other tissues including salivary and sweat glands, dendritic cells, skeletal and cardiac muscle, histiocytes, chondrocytes and lipocytes.[36,48–51]
S-100 remains the stain of choice for evaluating desmoplastic and spindle cell melanoma, but is less reliable than the aforementioned stains (HMB-45, Mel-5, and Melan-A) in recognizing epidermal melanocytic proliferation. However, S-100 has maintained its superiority in identifying the dermal component of melanomas.[35]
S-100 stains paraffin-embedded tissues better than frozen sections. Several studies have found S-100 to be problematic when used with frozen sections and noted S-100’s failure to identify melanoma or melanocytic hyperplasia,[34] decreased crispness, and increased background interference.[35] Despite this, S-100 is the stain of choice in MMS for the identification of melanomas with dermal components and desmoplastic melanoma.[34–36]
Conclusion
MMS is invaluable in the treatment of various aggressive and high-risk cutaneous neoplasms to achieve tumor-free margins. IHC as an adjunct to MMS facilitates identification of otherwise hard-to-delineate neoplastic cells, thereby increasing the procedure’s sensitivity. By harnessing the knowledge of the appropriate application of immunostains to specific tumors, the MMS surgeon is better equipped to maximize tissue sparing and minimize tumor recurrence. IHC offers a broad arena for continued research and further advances in MMS technique. We anticipate that continued use of IHC in MMS will enable the dermatology community to better serve their patients’ needs for both tumor-free survival and effective cosmesis.
References
1. Rapini RP. Comparison of methods for checking surgical margins. J Am Acad Dermatol. 1990;23:288–294.
2. Robinson, JK. Current histologic preparation methods for Mohs Micrographic Surgery. Dermatol Surg. 2001;27:555–560.
3. Polak JM, Van Noorden S. Introduction to Immunocytochemistry. 2nd ed. New York: Springer-Verlag; 1997.
4. Jimenez FJ, Grichnik JM, Buchanan MD, Clark RE. Immunohistochemical techniques in Mohs micrographic surgery: their potential use in the detection of neoplastic cells masked by inflammation. J Am Acad Dermatol. 1995;32(1): 89–94.
5. Zachary CB, Rest EB, Furlong SM, et al. Rapid cytokeratin stains enhance the sensitivity of Mohs micrographic surgery for squamous cell carcinoma. J Dermatol Surg Oncol. 1994;20(8):530–535.
6. Mondragon RM, Barrett TL. Current concepts: the use of immunoperoxidase techniques in Mohs micrographic surgery. J Am Acad Dermatol. 2000;43:66–71.
7. Jimenez FJ, Grichnik JM, Buchanan MD, Clark RE. Immunohistochemical techniques in Mohs micrographic surgery: their potential use in the detection of neoplastic cells masked by inflammation. J Am Acad Dermatol. 1995;32(1): 89–94.
8. Krunic AL, Garrod DR, Viehman GE, et al. The use of antidesmoglein stains in Mohs micrographic surgery. A potential aid for the differentiation of basal cell carcinoma from horizontal sections of the hair follicle and folliculocentric basaloid proliferation. Dermatol Surg. 1997;23(6):463–468.
9. Smeets NW, Stavast-Kooy AJ, Krekels GA, et al. Adjuvant cytokeratin staining in Mohs micrographic surgery for basal cell carcinoma. Dermatol Surg. 2003;29(4):375–377.
10. Luzi P, Miracco C, Del Vecchio MT, et al. Stereological study of desmosomes in basal cell carcinoma and seborrheic keratosis. J Submicrosc Cytol. 1987;19(2):337–343.
11. Mils V, Vincent C, Croute F, Serre G. The expression of desmosomal and corneodesmosomal antigens shows specific variations during the terminal differentiation of epidermis and hair follicle epithelia. J Histochem Cytochem. 1992;40(9): 1329–1337.
12. Ko CJ, McNiff JM, Glusac EJ. Squamous cell carcinomas with single cell infiltration: a potential diagnostic pitfall and the utility of MNF116 and p63. J Cutan Pathol. 2008;35(4):353–357.
13. Dotto JE, Glusac EJ. p63 is a useful marker for cutaneous spindle cell squamous cell carcinoma. J Cutan Pathol. 2006;33(6):413–417.
14. Ramnarain ND, Walker NP, Markey AC. Basal cell carcinoma: rapid techniques using cytokeratin markers to assist treatment by micrographic (Mohs) surgery. Br J Biomed Sci. 1995;52(3):184–187.
15. Garcia C, Clark RE, Buchanan M. Dermatofibrosarcoma protuberans. Int J Dermatol. 1996;35(12):867–871.
16. Ratner D, Thomas CO, Johnson TM, et al. Mohs micrographic surgery for the treatment of dermatofibrosarcoma protuberans. Results of a multi-institutional series with an analysis of the extent of microscopic spread. J Am Acad Dermatol. 1997;37(4):600–613.
17. Parker TL, Zitelli JA. Surgical margins for excision of dermatofibrosarcoma protuberans. J Am Acad Dermatol. 1995;32(2 Pt 1):233–236.
18. Garcia C, Viehman G, Hitchcock M, Clark RE. Dermatofibrosarcoma protuberans treated with Mohs surgery. A case with CD34 immunostaining variability. Dermatol Surg. 1996;22(2):177–179.
19. Karimipour DJ, Johnson TM, Kang S, et al. Mucinous carcinoma of the skin. J Am Acad Dermatol. 1997;36: 323–326.
20. Weber PJ, Hevia O, Gretzula JC, et al. Primary mucinous carcinoma. J Dermatol Surg Oncol. 1988;14(2):170–172.
21. Ortiz KJ, Gaughan MD, Bang RH, et al. A case of primary mucinous carcinoma of the scalp treated with Mohs surgery. Dermatol Surg. 2002;28(8):751–754.
22. Marra DE, Schanbacher CF, Torres A. Mohs micrographic surgery of primary cutaneous mucinous carcinoma using immunohistochemistry for margin control. Dermatol Surg. 2004;30(5):799–802.
23. Swanson SA, Cooper PH, Mills SE, et al. Lymphoepithelioma-like carcinoma of the skin. Mod Pathol. 1988;1(5):359–365.
24. Walker AN, Kent D, Mitchell AR. Lymphoepithelioma-like carcinoma in the skin. J Am Acad Dermatol. 1990;22(4): 691–693.
25. Glaich AS, Behroozan DS, Cohen JL, et al. Lymphoepithelioma-like carcinoma of the skin: a report of two cases treated with complete microscopic margin control and review of the literature. Dermatol Surg. 2006;32(2): 316–319.
26. Jimenez F, Clark RE, Buchanan MD, et al. Lymphoepithelioma-like carcinoma of the skin treated with Mohs micrographic surgery in combination with immune staining for cytokeratins. J Am Acad Dermatol. 1995;32: 878–881.
27. Chilukuri S, Page R, Reed JA, et al. Ectopic extramammary Paget’s disease arising on the cheek. Dermatol Surg. 2002;28(5):430–433.
28. Harris DW, Kist DA, Bloom K, et al. Rapid staining with carcinoembryonic antigen aids limited excision of extramammary Paget’s disease treated by Mohs surgery. J Dermatol Surg Oncol. 1994;20(4):260–264.
29. Coldiron BM, Goldsmith BA, Robinson JK. Surgical treatment of extramammary Paget’s disease. A report of six cases and a reexamination of Mohs micrographic surgery compared with conventional surgical excision. Cancer. 1991;67(4):933–938.
30. Murata Y, Kumano K, Tani M. Underpants-pattern erythema: a previously unrecognized cutaneous manifestation of extramammary Paget’s disease of the genitalia with advanced metastatic spread. J Am Acad Dermatol. 1999;40:949–956.
31. O’Connor WJ, Lim KK, Zalla MJ, et al. Comparison of Mohs micrographic surgery and wide excision for extramammary Paget’s disease. Dermatol Surg. 2003;29(7):723–727.
32. Smith KJ, Tuur S, Corvette D, et al. Cytokeratin 7 staining in mammary and extramammary Paget’s disease. Mod Pathol. 1997;10(11):1069–1074.
33. Dawn ME, Dawn AG, Miller SJ. Mohs surgery for the treatment of melanoma in situ: a review. Dermatol Surg. 2007;33:395–402.
34. Albertini JG, Elston DM, Libow LF, Smith SB, and Farley MF. Mohs micrographic surgery for melanoma: a case series, a comparative study of immunostains, an informative case report and a unique mapping technique. Dermatol Surg. 2002;28:656–665.
35. Zalla MJ, Lim KK, Dicaudo DJ, Gagnot MM. Mohs micrographic excision of melanoma using immunostains. Dermatol Surg. 2000;26:771–784.
36. Blessing K, Sanders DSA, Grant JJH. Comparison of immunohistochemical staining of the novel antibody Melan-A with S-100 protein and HMB-45 in malignant melanoma and melanoma variants. Histopathology. 1998;32:139–146.
37. Menaker GM, Chiang JK, Tabila B, Moy RL. Rapid HMB-45 staining in Mohs micrographic surgery for melanoma in situ and invasive melanoma. J Am Acad Dermatol. 2001;44(5): 833–836.
38. Robinson JK. Margin control for lentigo maligna. J Am Acad Dermatol. 1994;31:79–85.
39. Stonecipher MR, Leshin B, Patrick J, White WL. Management of lentigo maligna and lentigo maligna melanoma with paraffin-embedded tangential sections: utility of immunoperoxidase staining and supplemental vertical sections. J Am Acad Dermatol. 1993;29(4):589–594.
40. Griego RD, Zitelli JA. Mohs micrographic surgery using HMB-45 for a recurrent acral melanoma. Dermatol Surg. 1998;24: 1003–1006.
41. Gross EA, Anderson WK, Rogers GS. Mohs micrographic excision of lentigo maligna using mel-5 for margin control. Arch Dermatol. 1999;135:15–17.
42. de Vries TJ, Fourkour A, Wobbes T, et al. Heterogeneous expression of immunotherapy candidate proteins gp100, MART-1, and tyrosinase in human melanoma cell lines and in human melanocytic lesions. Cancer Res. 1997;57(15): 3223–3229.
43. Davis DA, Kurtz KA, Robinson RA. Ultrarapid staining for cutaneous melanoma: study and protocol. Dermatol Surg. 2005;31:753–756.
44. Bricca GM, Brodland DG, Zitelli JA. Immunostaining melanoma frozen sections: the one hour protocol. Dermatol Surg. 2004;30:403–408.
45. Hendi, A, Brodland DG, Zitelli JA. Melanocytes in long-standing sun-exposed skin. Arch Dermatol. 2006;142: 871–876.
46. Moore BW. A soluble protein characteristic of the nervous system. Biochem Biophys Res Comm. 1965;19:739–744.
47. Vanstapel MJ, Gatter KC, Wolf-Peeters C, et al. New site of human S-100 immunoreactivity detected with monoclonal antibodies. Am J Clin Pathol. 1986;85:160–168.
48. Takahashi K, Isobe T, Ohtsuki Y, et al. Immunohistochemical study on the distribution of alpha and beta subunits of S100 protein in human neoplasms and normal tissues. Virchows Arch (B). 1984;45:385–396.
49. Ruiter DJ, Brockner E. Immunohistochemistry in the evaluation of melanocytic tumors. Semin Diagn Pathol. 1993;10:76–91.
50. Wick MR, Swanson PE, Rocamora A. Recognition of malignant melanoma by monoclonal antibody HMB-45. An immunohistochemical study of 200 paraffin-embedded cutaneous tumors. J Cutan Pathol. 1988;15:201–207.
51. Ordonez NG, Xiaolong JI, Hickey RC. Comparision of HMB-45 monoclonal antibody and S-100 protein in the immunohistochemical diagnosis of melanoma. Am J Clin Pathol. 1988;90:385–390.