Jorge Garcia-Zuazaga, MD, MS; Malcolm Ke, MD; Director, Mohs Micrographic Surgery, University Hospitals Westlake Medical Center, Department of Dermatology, Case Western Reserve University, Cleveland, Ohio
Patrick Lee, MD, Division of Dermatology, University of California Los Angeles, Los Angeles, California
Abstract
Keratoacanthomas are fast-growing, solitary, cutaneous neoplasms that usually show spontaneous regression. The development of giant variants and aggressive behavior have been described. Clinically, a keratoacanthoma larger than 20 to 30mm is classified as a giant keratoacanthoma. A major challenge in dealing with these neoplasms is the difficulty of clinically and histologically differentiating them from squamous cell carcinoma. The authors report a practical approach using Mohs micrographic surgery for evaluation of large tumors. With this method, the lateral margins are evaluated and cleared prior to excision of the bulk of the tumor. The authors also describe alternative therapies for giant keratoacanthomas and present a case of a 61-year-old woman with a rapidly growing tumor on her left arm. Skin biopsy was consistent with a well-differentiated squamous cell carcinoma with focal features of a keratoacanthoma. The patient underwent Mohs micrographic surgery using the described approach, and no recurrence has been noted in four years. Surgical excision remains the treatment of choice for giant keratoacanthomas. Mohs micrographic surgery is a logical treatment option for giant keratoacanthomas. This case illustrates a useful approach that may prove valuable when treating large specimens during Mohs micrographic surgery. (J Clin Aesthetic Dermatol. 2009;2(8):22–25.)
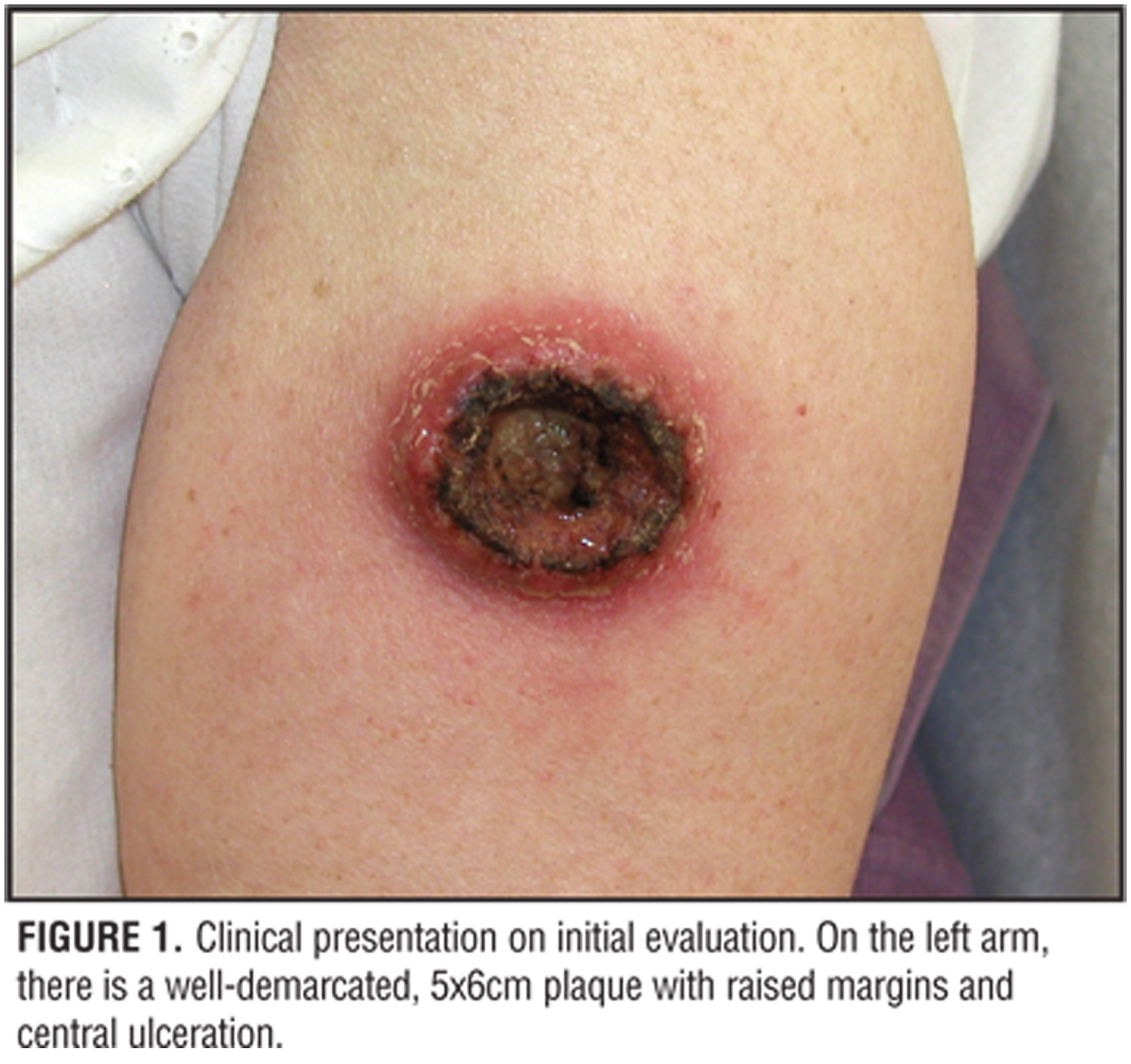
The authors present a case of a previously healthy 61-year-old Caucasian woman who presented to the dermatology clinic for evaluation of a rapidly growing exophytic tumor on her left arm. She first noticed the lesion two months prior to presentation and reported that it had nearly doubled in size over a period of three weeks. There was no history of trauma to the left arm. She had no significant past medical history and took no medications.
Physical examination revealed a well-demarcated, 5x6cm plaque with raised margins and central ulceration involving the left lateral arm (Figure 1). The overlying skin was diffusely erythematous. There was no evidence of regional lymphadenopathy or hepatosplenomegaly. The rest of the examination was unremarkable. All preoperative laboratory tests, including wound cultures, were unremarkable.
{kind=link}
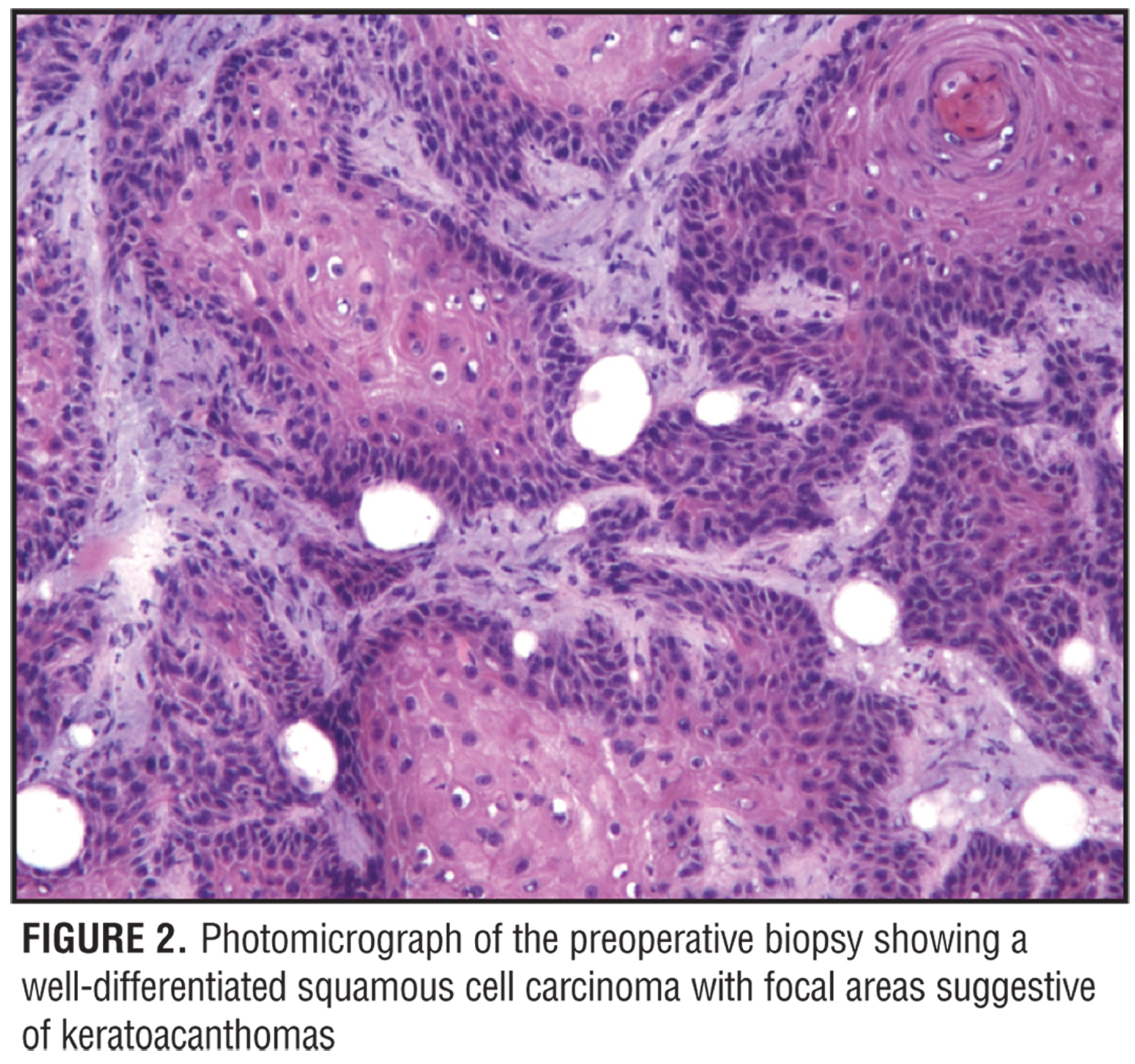
Preoperative biopsy revealed a well-differentiated squamous cell carcinoma (SCC) (Figure 2). Histologically, this tumor also shared features characteristic of a keratoacanthoma (KA) with squamous cell metaplasia, lymphohistiocytic infiltrate, and keratinocyte atypia.
{kind=link}
This case illustrates a distinct approach to the management of a giant KA using Mohs micrographic surgery (MMS) and summarizes the current treatment modalities for giant KAs.
Discussion
Keratoacanthomas are fast-growing, solitary, cutaneous neoplasms that usually show spontaneous regression.[1] Clinically, KAs tend to be solitary tumors usually seen on sun-exposed areas of lighter-skinned individuals. The most common locations include the face, forearms, and hands; its peak incidence is usually in the fifth decade.[1,2] The natural history of a KA involves three distinct stages as described by Schwartz: proliferative (rapid growth), mature (development of central keratinous core), and involution (necrosis and scarring).[1,2] The development of giant variants with aggressive and infiltrative behavior has been described in the literature. Clinically, a KA larger than 20 to 30mm is classified as a giant keratoacanthoma.[2,3]
The etiology of KAs is unknown, and many factors are likely involved in its pathogenesis.[1–4] It is assumed that KAs are derived from human hair follicles.[2,4] This observation has been supported by findings of follicular differentiation in keratin studies of KAs.[5] Furthermore, several investigators have reported that chronic ultraviolet radiation plays an important role in the development of solitary KA.[2–4] Other factors that may contribute to the pathogenesis of KAs include defects in DNA mismatch repair genes (as in the case of KAs developing in Muir-Torre Syndrome),[4] occupational exposure to chemical agents,[1,3,4] human papillomavirus (HPV) infection,[1,2,4] genetic alterations (bcl-2 proto-oncogene),6 and expression of the cyclin-dependent kinase inhibitor p27 in promoting regression of KAs.[7]
Keratoacanthomas create diagnostic and therapeutic dilemmas for the dermatological surgeon. A major challenge in dealing with these neoplasms is the difficulty of clinically and histologically differentiating them from SCC.[2,4,8] These tumors may have an unpredictable and aggressive course; some KAs may spontaneously regress in a period of months while others may behave like invasive SCC.
Multiple therapeutic modalities have been used for the treatment of KAs. Some of these modalities have included surgical excision,[9] such as MMS,[10,11] electrodessication and curettage,[1] intralesional corticosteroids,[1,2] topical and intralesional 5-fluorouracil,[12,13] systemic retinoids,[1,2] podophyllin,[1,2] radiation therapy,[1,2,4] interferon,[14] and methothrexate.[15–18] Most investigators advocate that each case be evaluated individually with respect to diagnosis and approach to treatment.
Excisional Surgery
For the majority of solitary KAs (including giant variants), excisional surgery is the treatment of choice.[1,2,9] Advantages of this modality include rapid treatment, definitive histopathological examination, prevention of local invasion and metastasis, and minimization of scarring, which may be significant post-involution.[19] Because of the difficulty of clinically and histologically differentiating KA from SCC, a fusiform excision, extending to the subcutaneous fat, that includes margins with normal skin and the center portion of the tumor is generally obtained. Recurrence rates ranging from 4 to 8 percent have been reported after surgical excision.[1–4] Substantial functional and cosmetic morbidity is a likely possibility depending on the anatomical location.
Mohs micrographic surgery. In this case, MMS was selected among other therapeutic modalities because of the dramatic size of the lesion requiring the need for tissue conservation, the presence of ill-defined borders on histology, and the lesser probability of recurrence.
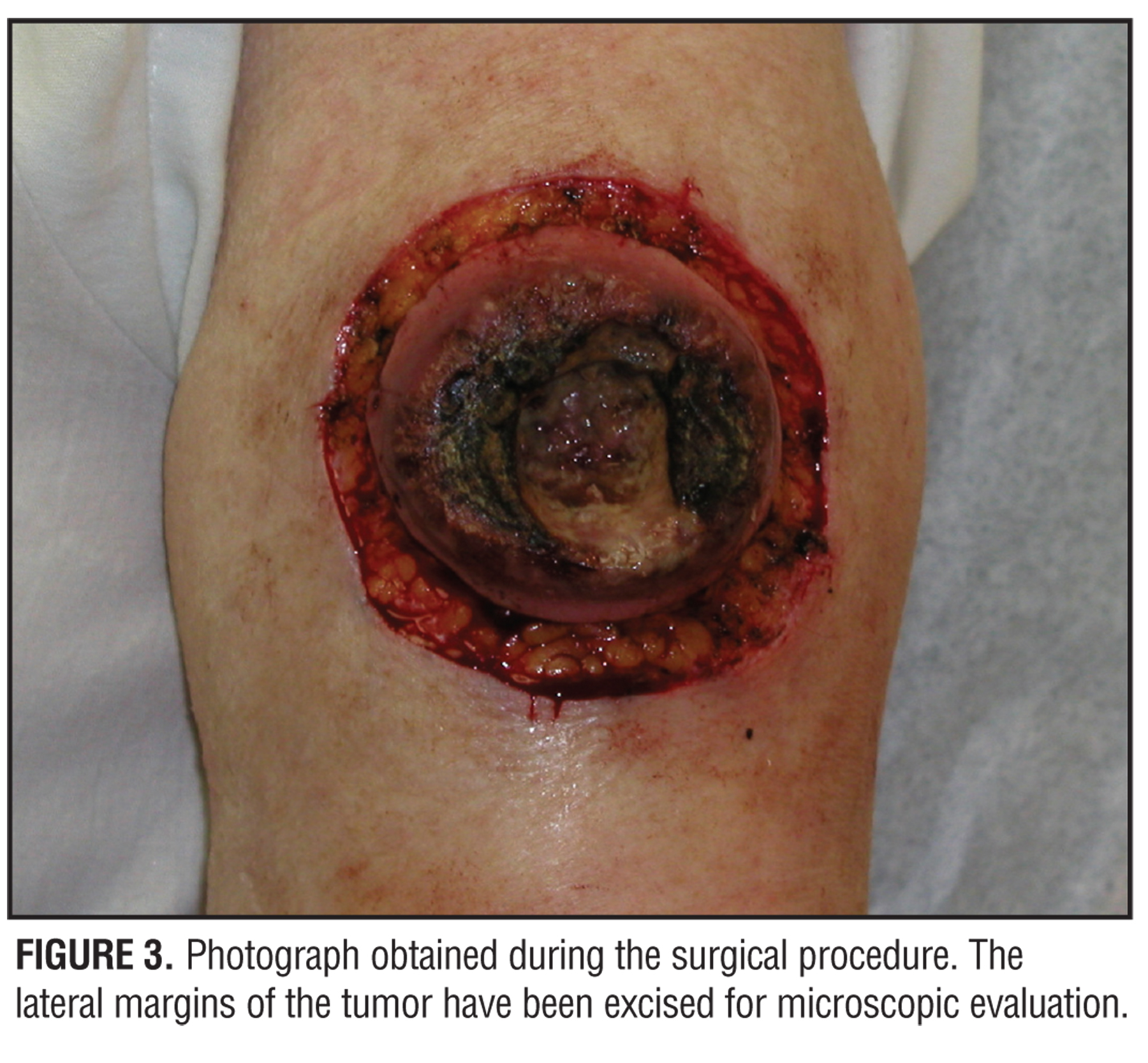
The patient underwent a three-stage, six-section, micrographically controlled excision. A slightly different approach was taken for the excision of this tumor. First, the lateral margin alone was obtained by means of an excision around the tumor with a clinical margin of normal-appearing tissue. This was mapped and processed lengthwise for full microscopic examination of the lateral margin (Figure 3). This process was repeated until the entire peripheral margin was clear of tumor. Excision of the deep margin and main bulk of the tumor followed. Once free of tumor, the surgical defect was repaired by a primary complex linear closure. For large specimens, the authors have found this technique very useful in maintaining accurate control of both the deep and lateral margins.
{kind=link}
MMS is considered an important alternative for patients with giant KA as well as those lesions involving the face or other critical anatomical locations.[10] This technique facilitates optimal margin control (microscopic surveillance of the complete perimeter of the specimen and contiguous deep margin) and conservation of normal tissue. Also, MMS provides prevention of rapid proliferation or impingement on important structures and improvement in overall cosmetic results.[11]
There are relatively few reports of KA treated with MMS in the literature. This may be due to the histological preference of calling KAs well-differentiated SCCs and grouping these cases into MMS for SCC. However, of those reported, recurrence rates using MMS have naturally been lower than by excisional surgery. In a series of 43 patients with KA treated with MMS, Larson reported a recurrence rate of 2.4 percent.[10]
Systemic and Topical Chemotherapy
Systemic chemotherapy has had variable results in the treatment of giant KAs. For multiple KAs and more aggressive KA variants, the use of systemic retinoids (etretinate 1mg/kg/day for 2 months) has been used successfully.[1,2]
Systemic methotrexate (MTX) has been used successfully in a subset of patients, namely those with large facial lesions involving the eyelid and lips and in patients with multiple KAs.[15,16] These studies postulate that by inhibiting dihydrofolate reductase (halting DNA synthesis), MTX may produce involution of KAs. Additionally, intralesional[16,17] and intramuscular administration of MTX has also been tried.[18] Observations from these reports recommend complete excision of any lesion that does not decrease in size after two MTX injections.[16,17]This approach could serve as adjuvant therapy to surgery or radiation for aggressive KAs.
5-fluorouracil (5-FU) has also been successful in the treatment of KAs. There are different reports of various techniques.[12,13] This approach has proven to be very favorable for large KAs in difficult-to-treat locations, such as the concha of the ear and nasal wall. However, it has been reported that 5-FU may not be as effective in treating KAs that are not rapidly proliferating.[2,13] This agent may be administered by either daily or every-other-day intralesional injection of a 5% solution directly onto the base of the KA for 2 to 3 weeks,[12] or by topical application of 5-FU up to five times a day.[12,13] Most lesions cleared in an average of 3 to 4 weeks following these protocols.[2,13,14,20]
Another chemotherapeutic agent used in the treatment of KAs is interferon (IFN) alpha-2a. Postulated mechanisms of action for IFN alpha-2a include antiproliferative effects, inhibiting epithelial cell differentiation, antiviral effects, and serving as an immunomodulator.[2,14] In 1993, Grobb et al reported regression with excellent cosmesis in five out of six patients treated with IFN alpha-2a.[14] In this open study, the authors used the dosage protocol similar to treatment of basal cell carcinomas. Initial treatment was 3×3 million units per week, which was increased to 3×6 million units per week. Side effects included pain at the injection site and transient fever after the first two injections. In five of the six cases, complete resolution was achieved in approximately five weeks with no recurrences noted at three years. Cosmetic results were described as excellent in four patients.
Radiation Therapy
Radiation therapy (RT) is rarely a first-line treatment for KA. It is more an alternative option reserved for cases of recurrent disease or as adjuvant therapy after surgery for giant KAs. It is also suitable for cases where surgery or other therapeutic modalities would be contraindicated and when resection would cause excessive deformity.[21]
There are no current established guidelines for RT for KA. Most authors recommend full cancericidal doses of 40 to 60Gy for giant KA. Disadvantages include frequent patient visits as well as cost. Side effects of RT include radiodermatitis, skin atrophy, and increased carcinogenic potential.[21,22]
Photodynamic Therapy
There are only anecdotal reports utilizing delta-aminolevulinic acid (ALA) photodynamic therapy (PDT) in the treatment of KA. Radakovic-Fijan et al reported complete resolution of lesions in four patients after two treatments using a 20% ALA emulsion under occlusion for more than 20 hours followed by irradiation using a 250W Osram halogen lamp and red filter (580–680 nm).[23] The authors utilized salicylic acid pretreatment of the tumor to facilitate ALA penetration and reported total exposure doses of 180J/cm2.[23] Complete remission was achieved four months after starting PDT and no signs of recurrence were seen at three years. Despite the lack of large studies using PDT for the treatment of KAs, observations by Fritsch et al that application of ALA induces selective porphyrin accumulation in skin neoplasms make PDT a suitable therapeutic alternative.[24]
Laser Therapy
Recently, ablative laser therapies have been successfully reported in the management of benign and malignant nonmelanocytic neoplasms. In 2004, Thiele et al reported successful treatment of a recurrent giant KA of the lower leg in a 64-year-old woman using the Er:Yag laser.[25] In this case report, the authors treated the lesion with pulse energies of 1000 to 2000mJ at 8Hz (spot size of 5mm) in four consecutive sessions with seven-day intervals. Immediately after laser treatment, 5-FU was topically applied to the treated area. There was no clinical evidence of recurrence six months after laser treatment. Interestingly, the Er:Yag laser has been shown to enhance transdermal delivery of both lipophilic and hypdrophilic drugs. The authors postulated that ablative laser pretreatment of the target area would disrupt the stratum corneum and improve delivery of 5-FU.[25]
Conclusion
Keratoacanthomas are fast-growing cutaneous neoplasms that usually show spontaneous regression. However, the development of giant variants with infiltrative and destructive behavior has been described. Surgical excision remains the treatment of choice for giant keratoacanthomas. MMS is a logical treatment option for giant KAs. This case illustrates a practical approach to clearing the lateral margins prior to removal of the bulk of the tumor. This technique may prove valuable when treating large specimens during MMS. Other therapeutic alternatives include systemic or topical chemotherapy (retinoids, methotrexate, 5-fluorouracil, interferon), radiation therapy, ablative laser therapy, and photodynamic therapy. Each case should be evaluated individually with respect to diagnosis and approach to treatment.
References
1. Schwartz RA. Keratoacanthoma. J Am Acad Dermatol. 1994;30(1):1–19.
2. Schwartz RA. Keratoacanthoma: a clinico-pathologic enigma. Dermatol Surg. 2004;30(2 Pt 2):326–333.
3. Pickrell K, Villarreal-Rios A, Neale H. Giant keratoacanthomas. Ann Plast Surg. 1979;3(2):172–176.
4. Bart RS, Popkin GL, Kopf AW, Gumport SL. Giant keratoacanthoma: a problem in diagnosis and management. J Dermatol Surg. 1975;1(2):49–55.
5. Smoller BR, Kwan TH, Said JW, Banks-Schlegel S. Keratoacanthoma and squamous cell carcinoma of the skin: immunohistochemical localization of involucrin and keratin proteins. J Am Acad Dermatol. 1986;14(2 Pt 1):226–234.
6. Sleater JP, Beers BB, Stephens CA, Hendricks JB. Keratoacanthoma: a deficient squamous cell carcinoma? Study of bcl-2 expression. J Cutan Pathol. 1994;21(6): 514–519.
7. Hu W, Cook T, Oh CW, et al. Expression of the cyclin-dependent kinase inhibitor p27 in keratoacanthoma. J Am Acad Dermatol. 2000;42(3):473–475.
8. Goldenhersh MA, Olsen TG. Invasive squamous cell carcinoma initially diagnosed as a giant keratoacanthoma. J Am Acad Dermatol. 1984;10(2 Pt 2):372–378.
9. Pagani WA, Lorenzi G, Lorusso D. Surgical treatment for aggressive giant keratoacanthoma of the face. J Dermatol Surg Oncol. 1986;12(3):282–284.
10. Larson PO. Keratoacanthomas treated with Mohs’ micrographic surgery (chemosurgery). A review of forty-three cases. J Am Acad Dermatol. 1987;16(5 Pt 1):1040–1044.
11. Shriner DL, McCoy DK, Goldberg DJ, Wagner RF Jr. Mohs micrographic surgery. J Am Acad Dermatol. 1998;39(1): 79–97.
12. Gray RJ, Medland NB. Topical 5-fluorouracil as primary therapy for keratoacanthoma. Ann Plast Surg. 2000;44(1): 82–85.
13. Parker CM, Hanke CW. Large keratoacanthomas in difficult locations treated with intralesional 5-fluorouracil. J Am Acad Dermatol. 1986;14(5 Pt 1):770–777.
14. Grob JJ, Suzini F, Richard MA, at al. Large kerato-acanthomas treated with intralesional interferon alfa-2a. J Am Acad Dermatol. 1993;29(2 Pt 1):237–241.
15. de Visscher JG, van der Wal KG, Blanken R, Willemse F. Treatment of giant keratoacanthoma of the skin of the lower lip with intralesional methotrexate: a case report. J Oral Maxillofac Surg. 2002;60(1):93–95.
16. Spieth K, Gille J, Kaufmann R. Intralesional methotrexate as effective treatment in solitary giant keratoacanthoma of the lower lip. Dermatology. 2000;200(4):317–319.
17. Melton JL, Nelson BR, Stough DB, et al. Treatment of keratoacanthomas with intralesional methotrexate. J Am Acad Dermatol. 1991;25(6 Pt 1):1017–1023.
18. Santoso-Pham JC, Shelley ED, Shelley WB. Aggressive giant keratoacanthoma of the face treated with intra-muscular methotrexate and triamcinolone acetonide. Cutis. 1997;59(6):329–332.
19. Edelman BA, Jacobs JB, Rotterdam H, Auerbach R. Giant keratoacanthoma: an atypical presentation. Otolaryngol Head Neck Surg. 1990;103(3):472–475.
20. Goette DK, Odom RB. Successful treatment of keratoacanthoma with intralesional fluorouracil. J Am Acad Dermatol. 1980;2(3):212–216.
21. Goldschmidt H, Sherwin WK. Radiation therapy of giant aggressive keratoacanthomas. Arch Dermatol. 1993; 129(9):1162–1165.
22. Donahue B, Cooper JS, Rush S. Treatment of aggressive keratoacanthomas by radiotherapy. J Am Acad Dermatol. 1990;23(3 Pt 1):489–493.
23. Radakovic-Fijan S, Honigsmann H, Tanew A. Efficacy of topical photodynamic therapy of a giant keratoacanthoma demonstrated by partial irradiation. Br J Dermatol. 1999;141(5):936–938.
24. Fritsch C, Batz J, Bolsen K, et al. Ex vivo application of delta-aminolevulinic acid induces high and specific porphyrin levels in human skin tumors: possible basis for selective photodynamic therapy. Photochem Photobiol. 1997;66(1):114–118.
25. Thiele JJ, Ziemer M, Fuchs S, Elsner P. Combined 5-fluorouracil and Er:YAG laser treatment in a case of recurrent giant keratoacanthoma of the lower leg. Dermatol Surg. 2004;30(12 Pt 2):1556–1560.