Cherie M. Ditre, MD, Assistant Professor of Dermatology, University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania
Editorial support for this article was provided by the editorial staff at Embryon. This article was funded by Dermik Laboratories, a business of sanofi-aventis U.S. The author gratefully acknowledges Patricia Bichler, PhD, who assisted in the preparation of this article based on author-provided comments. The opinions expressed in the current article are those of the author. The author received no honoraria or other form of financial support related to the development of this manuscript.
Abstract
Cheek implants may need to be removed from some patients due to pathologic conditions, such as infection, or patient dissatisfaction with cosmetic results. In these cases, correction of implant-associated facial volume loss may be achieved by using injectable poly-L-lactic acid. Injectable poly-L-lactic acid has been used successfully and safely for restoration and/or correction of the signs of facial fat loss (lipoatrophy) in people with human immunodeficiency virus. Here, the author reports the off-label use of injectable poly-L-lactic acid for the correction of facial volume loss following removal of malar cheek implants to yield a cheek lift and correction of prominent nasolabial fold wrinkles in a man with no significant medical problems. A total of three treatments using two vials of injectable poly-L-lactic acid per treatment were administered over the course of 16 weeks. Photographs were taken at baseline, during the 16-week injection period, and at a post-treatment evaluation visit 35 days after the final treatment (21 weeks after the initial injection). Although the patient has since been lost to follow up, he was very satisfied with the aesthetic results at the evaluation visit five weeks after the last treatment and expressed a desire to be treated with poly-L-lactic acid in the future. Injectable poly-L-lactic acid may be a good option for the correction of facial volume loss due to reasons other than human immunodeficiency virus-related lipoatrophy. (J Clin Aesthetic Dermatol. 2009;2(6):32–35.)
According to a survey of board-certified plastic surgeons, dermatologists, and otolaryngologists, almost 35,000 patients in the United States had facial cosmetic procedures involving injectable poly-L-lactic acid (PLLA) in 2007.[1] In the same year, 2,400 patients underwent surgical cheek implant placement. Approximately 10 to 12 percent of facial implants may need to be removed due to postsurgical complications (e.g., infection)[2] or incorrect implant size, shape, or position.[3] Nerve and blood vessel injury, persistent swelling, and hematoma have also been reported as complications of implants, although these do not always require implant removal.[4] Removal of permanent cheek implants often results in depressions in the malar region secondary to implant-induced bone erosion and soft-tissue contracture.[3] Injectable PLLA has been used to restore and/or correct the signs of facial fat loss (lipoatrophy) in people with human immunodeficiency virus (HIV) and has demonstrated an excellent safety and tolerability profile.[5–7] Injectable PLLA is currently under review by the United States Food and Drug Administration for volume restoration and/or correction of moderate-to-deep facial wrinkles and folds, such as nasolabial lines or folds. This report describes the cosmetic use of injectable PLLA for the correction of facial volume loss following removal of malar cheek implants in a man with no significant medical conditions and should therefore be considered an off-label use of the product.
Case Report
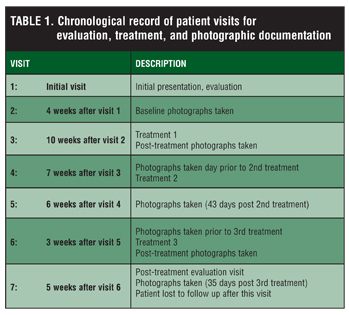
A 23-year-old man presented to the author’s practice for a cosmetic consultation and one month later for baseline photographic documentation (Table 1). The patient had a history of cheek implants that had been removed prior to presentation. He denied any specific disease process underlying the contour deficiency that led to malar implant surgery, but noted that he had a cleft palate as a child. The patient also denied any previous treatment with other skin rejuvenation products. On examination, he had flattened facies with depression of the malar eminences and consequent prominent nasolabial fold wrinkles. Several options were discussed with the patient, including agents that increase volume, such as fat, injectable PLLA, filler substances (i.e., hyaluronic acid derivatives), and collagen. The patient opted for treatment with injectable PLLA.
{kind=link}
Treatment Overview
Injectable PLLA was administered during three treatment sessions over approximately a four-month period. During each session, two vials of injectable PLLA were administered. A greater-than-normal volume of injectable PLLA was used in this patient due to the contour deficiency resulting from removal of cheek implants. Each vial was reconstituted the night before by using 5mL of sterile water for injection (SWFI).[8] The morning of the procedure, 2mL of 2% lidocaine were added to each vial. This reconstitution procedure differs from the method described in the product insert, which specifies reconstitution with 5mL of SWFI at least two hours before use. Lidocaine 4% cream (Elamax™, Ferndale Laboratories, Ferndale, Michigan) was applied to the injection site before treatment in order to reduce pain. Nearly all of the total reconstitution volume of 6.5mL in each vial was recovered, so the patient received about 13mL at each treatment. During the procedure, the patient was placed in a sitting position with his legs elevated on the table. The injections were made with a 26-gauge needle, using a threading or tunneling technique. At least 5.5mL were injected into each malar cheek, and the remaining 1mL per vial was injected into the nasolabial folds. The needle was introduced bevel up into the skin at a 30- to 40-degree angle.[8] When the appropriate deep dermal plane was reached, thin threads of injectable PLLA were deposited superiorly and laterally using a threading or tunneling technique. Injections were repeated until the full amount had been injected. Ice was subsequently applied to the site to reduce swelling while avoiding direct contact of the ice with the skin.
The patient received written postprocedure instructions after a registered nurse reviewed them with him. Specifically, the nurse reminded him to apply ice to the treated area (avoiding direct contact with the skin) for the first 8 to 12 hours to keep swelling at a minimum, and stressed the importance of massaging the treated area for five minutes five times per day for five days following treatment to evenly distribute the product.[9] While no clinical studies have formally examined the optimal frequency of massage, many practitioners believe that massage may result in a more homogenous distribution of the product.9 The patient verbalized his understanding of these instructions.
As recorded in Table 1, photographs were taken at baseline, immediately after the first treatment, prior to the second treatment, 43 days after the second treatment, before and immediately after the third treatment, and 35 days after the third treatment. Treatment results were evaluated by photographic documentation and patient self-assessment. The patient reviewed the results during the procedure and was given an opportunity to view and compare his baseline photograph with the post-treatment photographs (Figure 1). At the post-treatment evaluation visit five weeks after the final treatment, the patient reported that he was very satisfied with the results of his treatment. Although the patient was lost to follow up after this visit, he reported no adverse events over the five-month span from the beginning of the injection period to the post-treatment evaluation visit.
{kind=link}
Discussion
In some cases, malar implants must be removed because of infection or unacceptable cosmetic outcomes.[2,3] Although injectable PLLA is currently approved for the correction of facial fat loss (lipoatrophy) in people with HIV, it is pending approval for volume restoration and/or correction of facial wrinkles and folds, such as nasolabial lines or folds. In the case reported here, a patient with no significant medical problems desired a durable, but not permanent, volume correction and, after counseling by his physician, chose injectable PLLA. Recent studies have shown that increases in dermal thickness resulting from treatment of lipoatrophy in people with HIV who use injectable PLLA are detectable for up to two years.[6,7,10] In my clinical experience, facial volume correction achieved with injectable PLLA is maintained for approximately 2 to 3 years. While it is difficult to compare the duration of dermal fillers in the absence of direct comparative studies, the duration of effect for injectable PLLA is generally considered to be longer than that of currently available injectable devices, including collagens (approximately three months for older collagen products and up to one year for more recently available porcine collagen),[11,12] hyaluronic acids (six months to more than one year depending on the product and location of use),[11,13–16] and calcium hydroxylapatite (one year or longer).[11,17] Thus, the sustained duration of injectable PLLA may be most appropriate for patients electing to pursue longer-term, but nonpermanent, correction of facial volume deficits.
Although follow up of this patient after the final treatment session was limited to 35 days, the treatment appears to have been well tolerated. The patient reported no adverse events over the five months following the initial treatment session with injectable PLLA. In a long-term study of safety and efficacy of injectable PLLA, the vast majority of treatment-related adverse events were reported at the time of injection and all were localized to the injection site.[6] Adverse events reported other than at the time of injection included one case of infection (reported two weeks after the first injection), one case of injection-site induration, and nine cases of injection-site nodules (described as “lumps” or “bumps” that were palpable, but generally nonvisible). Woerle et al have reported a tenfold reduction in the incidence of subcutaneous papules that coincided with a switch to reconstituting injectable PLLA with a total volume of 5mL rather than 3mL as used in the Moyle study.[18] Since the early clinical trials of injectable PLLA, other refinements in the reconstitution,[9] injection technique,[19] and post-treatment massage[20] have been postulated to decrease the incidence of nodules or subcutaneous papules.[21] Nonetheless, physicians should be aware of the potential for late-onset subcutaneous nodules, some of which (overall incidence as low as 0.1%) have been characterized by histology as foreign-body granulomas.[22–25]
In summary, this patient achieved a very satisfactory correction of facial volume following removal of malar cheek implants and did not report any adverse events throughout the 16-week treatment period or the five-week post-treatment period. The patient was impressed with the aesthetic results obtained using injectable PLLA and expressed a desire for retreatment with the product, when necessary. Experience with injectable PLLA with respect to reconstitution, injection technique, and post-treatment patient instruction has facilitated the ability of physicians to optimize outcomes in patients.
References
1. American Society for Aesthetic Plastic Surgery. Cosmetic Surgery National Data Bank Statistics. 2007;1–20.
2. Wang TD. Multicenter evaluation of subcutaneous augmentation material implants. Arch Facial Plast Surg. 2003;5(2):153–154.
3. Yaremchuk MJ. Secondary malar implant surgery. Plast Reconstr Surg. 2008;121(2):620–628.
4. Lowe NJ, Grover R. Injectable hyaluronic acid implant for malar and mental enhancement. Dermatol Surg. 2006;32(7):881–885.
5. Mest DR, Humble G. Safety and efficacy of poly-L-lactic acid injections in persons with HIV-associated lipoatrophy: the US experience. Dermatol Surg. 2006;32(11):1336–1345.
6. Moyle GJ, Brown S, Lysakova L, Barton SE. Long-term safety and efficacy of poly-L-lactic acid in the treatment of HIV-related facial lipoatrophy. HIV Med. 2006;7(3):181–185.
7. Valantin MA, Aubron-Olivier C, Ghosn J, et al. Polylactic acid implants (New-Fill) to correct facial lipoatrophy in HIV-infected patients: results of the open-label study VEGA. AIDS. 2003;17(17):2471–2477.
8. Sculptra [package insert]. Bridgewater, NJ: Dermik Laboratories, a business of sanofi-aventis U.S. LLC; 2006.
9. Beer KR, Rendon MI. Use of Sculptra™ in esthetic rejuvenation. Semin Cutan Med Surg. 2006;25(3): 127–131.
10. Burgess CM, Quiroga RM. Assessment of the safety and efficacy of poly-L-lactic acid for the treatment of HIV-associated facial lipoatrophy. J Am Acad Dermatol. 2005;52(2):233–239.
11. Dayan SH, Bassichis BA. Facial dermal fillers: selection of appropriate products and techniques. Aesthetic Surg J. 2008;28(3):335–347.
12. Evolence collagen filler [package insert]. Herzliya, Israel: ColBar LifeScience, Ltd.; 2008.
13. JuveDerm® 24HV [package insert]. Paris, France: Corneal; 2006.
14. Juvederm™ Ultra Plus [package insert]. Pringy, France: Allergan; 2008.
15. Perlane® [package insert]. Scottsdale, Arizona: Medicis Aesthetics, Inc.; 2007.
16. Restylane® [package insert]. Scottsdale, Arizona: Medicis Aesthetics, Inc.; 2007.
17. Radiesse Injectable implant [package insert]. Franksville, Wisconsin: BioForm Medical Inc.; 2006.
18. Woerle B, Hanke CW, Sattler G. Poly-L-lactic acid: a temporary filler for soft tissue augmentation. J Drugs Dermatol. 2004;3(4):385–389.
19. Borelli C, Kunte C, Weisenseel P, et al. Deep subcutaneous application of poly-L-lactic acid as a filler for facial lipoatrophy in HIV-infected patients. Skin Pharmacol Physiol. 2005;18(6):273–278.
20. Lowe NJ. Optimizing poly-L-lactic acid use. J Cosmet Laser Ther. 2008;10(1):43–46.
21. Sadick NS. Poly-L-lactic acid: a perspective from my practice. J Cosmet Dermatol. 2008;7(1):55–60.
22. Reszko AE, Sadick NS, Magro CM, Farber J. Late-onset subcutaneous nodules after poly-L-lactic acid injection. Dermatol Surg. 2009;35(Suppl 1):380–384.
23. Beer K. Clinicopathologic correlation of delayed-onset periorbital poly-L-lactic acid nodules. Dermatol Surg. 2009;35(Suppl 1):399–402.
24. Christensen L, Breiting V, Janssen M, et al. Adverse reactions to injectable soft tissue permanent fillers. Aesthetic Plast Surg. 2005;29(1):34–48.
25. Bauer U, Vleggaar D. Response to “New-fill injections may induce late-onset foreign body granulomatous reaction.” Plast Reconstr Surg. 2006;118(1):265–266.