 J Clin Aesthet Dermatol. 2021;14(3):30–31.
J Clin Aesthet Dermatol. 2021;14(3):30–31.
by Federica Scarfì, MD; Flavia Silvestri, MD; Luciana Trane, MD; Alessia Gori, MD; Federico Venturi, MD; and Vincenzo De Giorgi, MD
Drs. Scarfì, Silvestri, Trane, Venturi, and De Giorgi are with the Department of Dermatology, University of Florence in Florence, Italy. Dr. Gori is with the Cancer Research Attilia Pofferi Foundation in Pistoia, Italy.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors report no conflicts of interest relevant to the content of this article.
ABSTRACT: Cutaneous lesions of vascular origin are normally easily diagnosed, both clinically and dermoscopically. However, Kaposi’s sarcoma can trigger difficulties in making a correct preoperative diagnosis. Although dermoscopic pictures are not pathognomonic for diagnosing Kaposi’s sarcoma, dermoscopic analysis could be a useful complement to a differential diagnosis of nodular pigmented cutaneous lesions. Here, we discuss two clinical cases and analyze the primary dermoscopic features of Kaposi’s sarcoma, evaluating the potential utility of this method for differential diagnosis.
Keywords: Cutaneous lesions, dermoscopy, Kaposi’s sarcoma
A 66-year-old man presented to our clinic with three nodular lesions located on the external surface of his right ear. The lesions had appeared about five years prior and exhibited slow but progressive growth, with one in particular growing significantly, changing color, and differentiating during the most recent six months. The patient had no personal or family history of skin tumors and no medical history of sexually transmitted diseases. The patient was negative for human immunodeficiency virus and showed no associated immunosuppression. A routine blood test and renal and liver function tests were within normal limits.
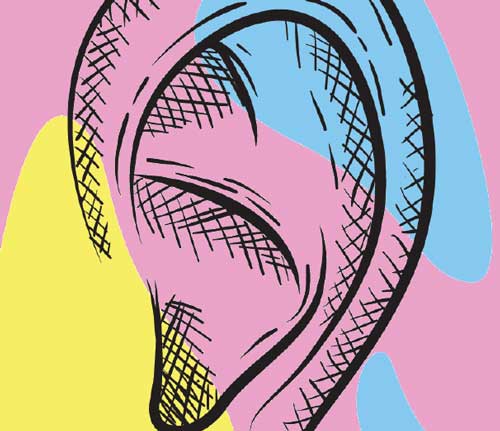
Upon physical examination, a painless reddish nodule, raised above the skin by about 5mm and surrounded within about 1cm by small, dark, palpable satellite lesions was identified on the back of the right ear (Figure 1).
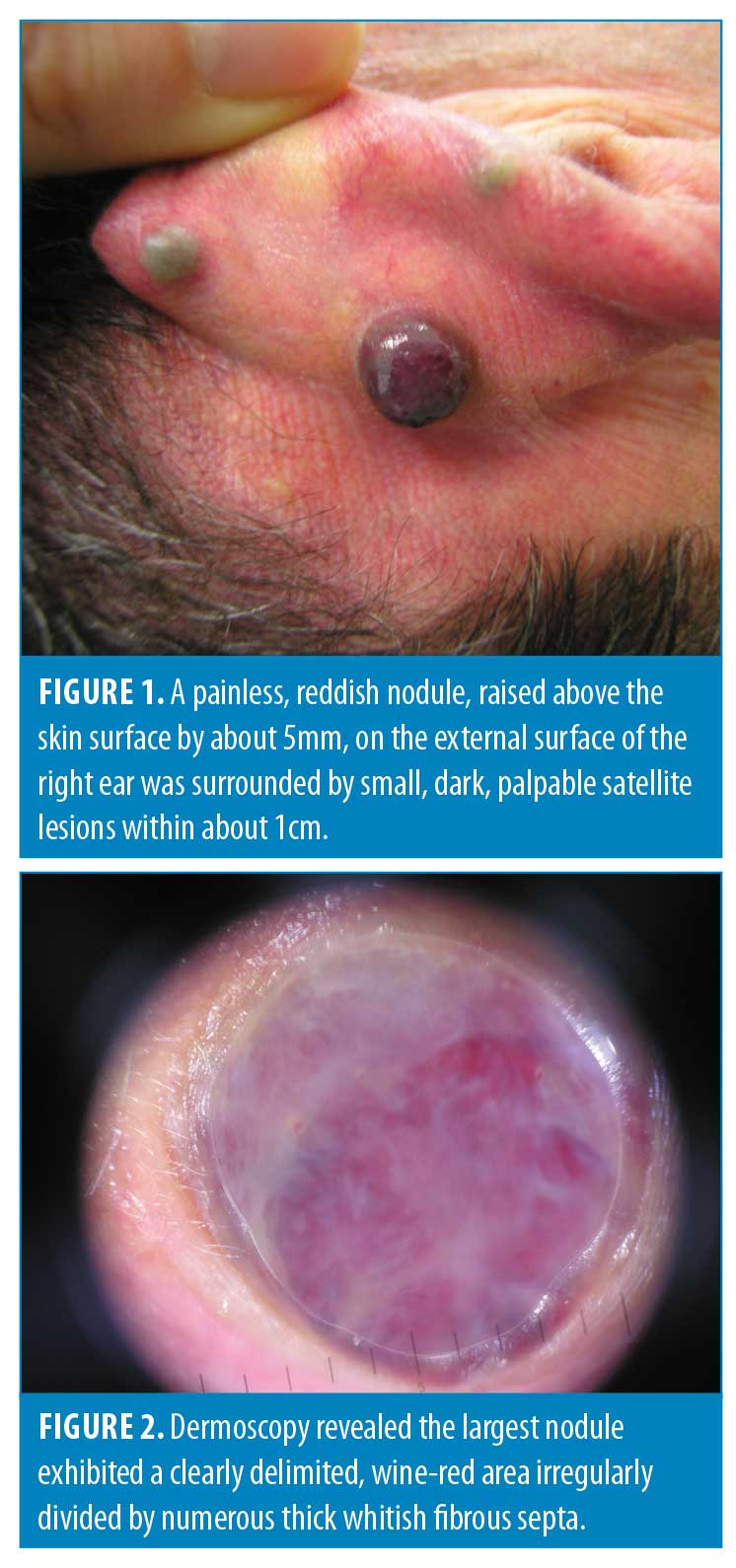
A dermoscopic image of the largest lesion featured a clearly bluish-reddish, delimited area irregularly divided by numerous thick, whitish, fibrous septa and a weak focal iridescence (Figure 2). A dermoscopic image of the smallest lesions showed a homogeneous blue area with clearly defined and regular limits (Figure 3). No other parameters were noted. The clinical and dermoscopic findings were suggestive of vascular lesions, but a diagnosis of nodular melanoma with satellitosis could not be ruled out considering the patient’s history and the nonspecific clinical characteristics of the lesions.

The lesions were surgically removed by excisional biopsy and histological examinations commenced. The largest lesion proved to be Kaposi’s sarcoma, while the others were diagnosed as hemangiomas.
Similar lesions were not found in any other region of the body. The abdomen and thorax were evaluated using computerized tomography and results were negative. The patient did not receive other treatment aside from surgical excision of the lesions.
The postoperative course was free of complications and the patient was clinically disease-free at the two-year follow up.
Discussion
Kaposi’s sarcoma is clinically suspected and histologically confirmed—an easy task in the majority of cases where the skin lesions have a distinctive color and typical distribution at clinical presentation. Several conditions should be considered in a differential diagnosis, particularly when evaluating a single pigmented lesion, such as hemangioma, angiokeratoma, pyogenic granuloma, melanocytic lesion, lymphangioma, or lymphangiosarcoma. Most of these prove to be of vascular origin, giving them very similar morphological aspects.
In the present case, the rapid appearance of multiple lesions mimicked a melanocytic satellitosis that was difficult to classify. Additionally, the possible metastasis and the blue nevus satellitosis generated well-founded concerns.1,2 For these reasons, we analyzed the lesions dermoscopically to increase the accuracy of our preoperative diagnosis. The dermoscopic analysis of the largest nodule, a reddish area irregularly divided by numerous thick, whitish septa and with a weak focal iridescence, proved to be nonspecific even though it presented with similar features to those of vascular lesions, particularly of angiokeratomas. Indeed, those lesions were characterized by red or blue areas clearly delimited by fibrous septa constituting a global lacunar pattern. The nodule tended to show focal iridescence that could resemble a rainbow pattern as first described by Hu et al.3,4
Although the rainbow pattern was initially thought to be specific to Kaposi’s sarcoma, it has been reported in non-Kaposi’s lesions, such as melanoma, blue naevi, basal cell carcinoma, atypical fibroxanthomas, scar tissue, stasis dermatitis, and others.5–8 Vázquez-López et al5 postulated that the rainbow effect occurs when light in different states of polarization interacts with the structures of the lesions (i.e., dichroism) and not from light diffraction occurring through structural arrangement of vessels in Kaposi’s sarcoma, as previously suggested.4
The dermoscopic pattern of Kaposi’s sarcoma with a reddish area, whitish septa, and lack of a clear rainbow pattern was noted in our case, even though the rainbow is seen in the majority, but not all (71%), of papular and nodular lesions.9 Our experience and the literature suggests that this type of pattern is more common in recently formed lesions and those characterized by rather rapid evolution. Another case involved nodular Kaposi’s sarcoma, almost four years prior, on the back of the hand of a 78-year-old man. In that case, the dermoscopic imaging showed a homogeneous bluish pigmentation with a purplish hue (Figure 4), a characterization more frequently found in older, slower-growing lesions.10

The present case was extremely challenging because the differential diagnosis was confounded by the blue nevus and nodular melanoma. The dermoscopic differences in patterns could be linked to the physiological evolution of nodular Kaposi’s sarcoma, which tends to include coalescence, erosion, and ulceration.
Conclusion
In our experience, nodular Kaposi’s sarcoma can have two primary dermoscopic features linked to its normal evolution: one is a reddish area irregularly divided by numerous thick, whitish fibrous septa and a rainbow pattern (in younger lesions) and the other is a homogeneous bluish pigmentation with a purplish hue, possibly accompanied by superficial scales (in longer-standing lesions). A dermoscopic feature common to both is a peculiar bluish-reddish area, present at varying extents, seemingly typical of nodular Kaposi’s sarcoma.
Although these dermoscopic images are not pathognomonic for the diagnosis of nodular Kaposi’s sarcoma, they could be useful complements in the differential diagnosis of nodular pigmented cutaneous lesions.
References
- Sahin MT, Demir MA, Yoleri L, et al. Blue naevus with satellitosis mimicking malignant melanoma. J Eur Acad Dermatol Venereol. 2001;15(6):570–573.
- Goldenhersh MA, Savin RC, Barnhill RL, Stenn KS. Malignant blue nevus. Case report and literature review. J Am Acad Dermatol. 1988;19(4):712–722.
- Cheng ST, Ke CL, Lee CH, et al. Rainbow pattern in Kaposi’s sarcoma under polarized dermoscopy: a dermoscopic pathological study. Br J Dermatol. 2009;160(4):801–809.
- Hu SC, Ke CL, Lee CH, et al. Dermoscopy of Kaposi’s sarcoma: areas exhibiting the multicoloured ‘rainbow pattern’. J Eur Acad Dermatol Venereol. 2009;23(10):1128–1132.
- Vázquez-López F, García-García B, Rajadhyaksha M, Marghoob AA. Dermoscopic rainbow pattern in non-Kaposi sarcoma lesions. Br J Dermatol. 2009;161(2):474–475.
- Pinos León VH, Granizo Rubio JD. Acral pseudolymphomatous angiokeratoma of children with rainbow pattern: a mimicker of Kaposi sarcoma. J Am Acad Dermatol. 2017;76(2S1):S25–S27.
- Pérez-Pérez L, García-Gavín J, Allegue F, Zulaica A. The rainbow pattern and rosettes in cutaneous scars. Actas Dermosifiliogr. 2014;105(1):96–97.
- Uzunçakmak TK, Ozkanli S, Karada? AS. Dermoscopic rainbow pattern in blue nevus. Dermatol Pract Concept. 2017;7(3):60–62.
- Satta R, Fresi L, Cottoni F. Dermoscopic rainbow pattern in Kaposi’s sarcoma lesions: our experience. Arch Dermatol. 2012;148(10):1207–1208.
- Scope A, Benvenuto-Andrade C, Agero AL, Marghoob AA. Non melanocytic lesions defying the two-step dermoscopy algorytm. Dermatol Surg. 2006;32(11):1398–1406.