Sherrie J. Divito, PhD; Justin M. Haught, MD;
Joseph C. English, III, MD; Laura K. Ferris, MD, PhD
Department of Dermatology, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania
Abstract
Dermonecrotic arachnidism is the potential cutaneous reaction to spider bite venom. The yellow sac spider, genus Cheiracanthium, is historically considered capable of inducing dermonecrotic lesions. However, recently this belief has been hotly debated. In this article, the authors provide a brief review of dermonecrotic arachnidism and describe a case of a 20-year-old man who developed severe necrosis and edema of the left thigh, buttock, penis, and scrotum following the bite of a yellow sac spider. Notably, the patient wore a tight-fitting garment for multiple hours following the spider bite, thus compressing the envenomated tissue. This is the first case reporting such severe dermonecrosis resulting from a yellow sac spider bite and highlights the potential effects of tissue compression following spider envenomation.
(J Clin Aesthetic Dermatol. 2009;2(9):40–43.)
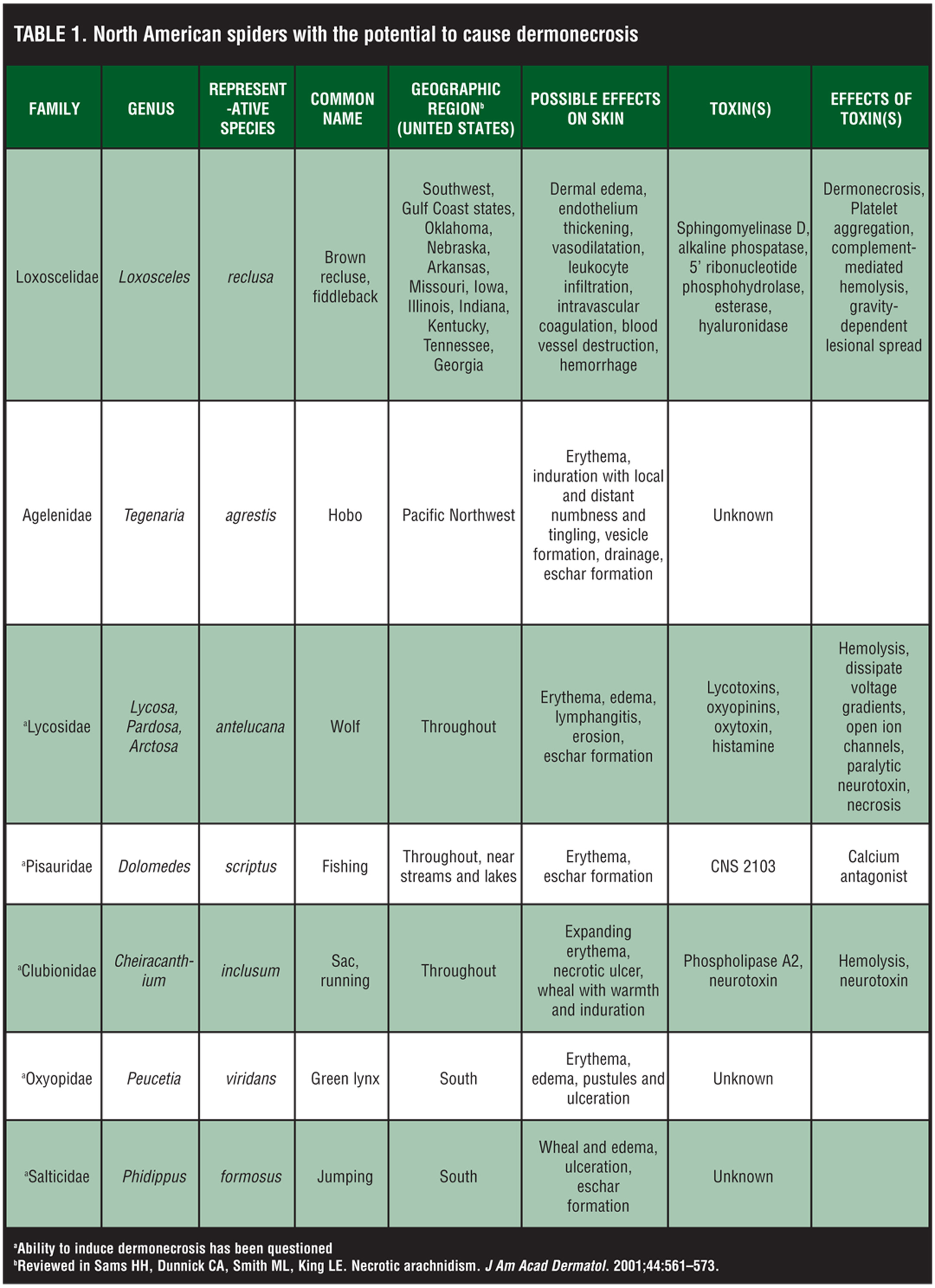
Dermonecrotic arachnidism is the potential cutaneous reaction to spider bite venom, and it manifests typically as vasodilatation, ischemia, and thrombosis or “red, white, and blue sign.” In the United States, there are seven spider families considered capable of inducing clinically relevant dermonecrotic lesions (Table 1),[1] and although there are roughly 10,000 spider bites reported to poison control centers nationwide each year,2 diagnosis of dermonecrotic arachnidism is difficult, particularly since positive spider identification is rarely made. As a result, diagnosis and reports of spider bites in the literature have become a point of controversy for dermatologists and entomologists.
{kind=link}
Further complicating matters, the ability of many of these spiders—including the wolf (Lycosa, Pardosa, Arctosa), green lynx (Peucetia), jumping (Phidippus), fishing (Dolomedes), and yellow sac (Cheiracanthium) spiders—to induce necrosis has recently been questioned (Table 1). Only Loxosceles venom (from the brown recluse spider) has been demonstrated to contain a toxin, sphingomyelinase D, capable of inducing ulceration. In addition, sphingomyelinase D also causes platelet aggregation and complement-mediated hemolysis.[3] Lesions are characterized by dermal edema, endothelial thickening, vasodilatation, leukocyte infiltration, intravascular coagulation, blood vessel destruction, and hemorrhage.[3] The hobo spider (Tegenaria) is the leading cause of necrotic arachnidism in the Northwest, although the contents of its venom are unknown.[2,4] The ability of those toxins identified within venoms of the other spiders (Table 1)[5–8] to induce dermal necrosis has not been confirmed. The potential skin manifestations induced by spider bites is summarized in Table 1.[1]
The yellow sac spider, genus Cheiracanthium, is classically considered by dermatologists as capable of inducing dermonecrosis.[1] Two species are found in the United States, C inclusum and C mildei. These spiders are about 7.5mm in length,[9] do not spin webs, and tend to come indoors in the fall and winter in search of food. Cheiracanthium envenomation has historically been thought to result in expanding erythema associated with pruritus and pain lasting roughly three days, with potential formation of a shallow necrotic ulcer in the first day and an average healing time of 10 to 14 days.[10] Recently however, researchers have begun to question the ability of Cheiracanthium to induce dermonecrosis.[11] In this article, the authors present a 20-year-old man who developed extensive dermonecrosis requiring split-thickness skin grafting following a yellow sac spider bite, which potentially resulted from compression of the envenomated tissue by tight-fitting garments.
Case Report
A previously healthy 19-year-old man presented to the authors’ office in the fall from an outside hospital with extensive red and purple discoloration, pain, and swelling of the left thigh extending into the scrotum, penis, and lower left abdomen. He experienced acute onset pruritus of the left anterior thigh shortly after putting on his football uniform prior to a game. He reported no trauma during the game. After removing his uniform three hours later, he noticed the skin changes. Physical examination revealed edema, purpura, and skin sloughing of the left anterior thigh extending into the left buttock, penis, scrotum, and lower left abdomen without crepitus (Figure 1a and Figure 1b). Magnetic resonance imaging revealed extensive edema from the level of the left iliac crest to the left knee without fascial plane involvement, fluid collections, or subcutaneous gas (Figure 2). Incision with subsequent digital probing did not show evidence of necrotizing fasciitis or infection. Tissue culture was negative. Laboratory testing revealed a leukocytosis of 18.4 with a left shift (bands 16%) and high neutrophil count (69%). Deep punch biopsy revealed a diffuse neutrophilic infiltrate with eosinophils and necrosis of the dermis, follicles, eccrine glands, and portions of the subcutis. It was later discovered that the locker room was “infested” with spiders. One of these spiders was collected and identified by an entomologist as belonging to the genus Cheiracanthium. Given the history, presentation, laboratory testing, and histopathology, a diagnosis of dermonecrotic arachnidism was made. Intravenous broad-spectrum antibiotics, supportive care, and debridement with split-thickness skin grafting were instituted with good clinical outcome.
{kind=link}
{kind=link}
{kind=link}
Discussion
There is a wide differential diagnosis for necrotic arachnidism (Table 2).[1] Classification of spider bites is based on history and presentation. Spider bites are classified as putative, presumptive, probable, and documented.[1] A documented bite requires immediate spider collection and positive identification, which rarely occurs.
In this case, although a spider was not recovered at the time of the bite, the team’s locker room was infested with yellow sac spiders, as identified by a knowledgeable entomologist. Interestingly, the ability of Cheiracanthium to induce dermonecrosis is disputable. Although Cheiracanthium envenomation in guinea pigs results in necrotic lesions,[12] whether these findings translate to humans is unclear, and reports of human victims with necrotic lesions attributed to Cheiracanthium bites are numerous but circumstantial,[12–13] as the responsible spider has never been actually verified. A prospective study demonstrated that of 20 patients bitten by a Cheiracanthium spider, none experienced dermonecrosis,[11] and the study’s authors recognized from the literature only one verified Cheiracanthium bite responsible for causing a small necrotic lesion.[14]
Consistent with a Cheiracanthium bite, the patient described in this case was bitten in the Fall, while dressing, and experienced localized pruritus—a common early symptom.[11] Notably, other dermonecrotic-causing arachnids including the brown recluse, hobo, green lynx, and jumping spiders, are not indigenous to this geographic region. This information coupled with the confirmed Cheiracanthium infestation of the locker room where the bite occurred suggests a classification of a “probable” bite by a yellow sac spider,[1] although the clinical presentation is certainly atypical.
Treatment for spider bites is typically the same regardless of the causative spider. Rest, ice compresses, and elevation, or “RICE” therapy, are the mainstay of treatment whenever a spider bite is suspected.[15,16] Antibiotics to prevent secondary infection and analgesics may be indicated. Tetanus booster, if due, and antihistamines may also be appropriate. In the setting of Loxoscelism (the medical syndrome caused by bites of recluse spiders), dapsone treatment may be beneficial for moderate-to-severe dermonecrosis,[17] as dapsone has numerous modulatory effects on neutrophil migration and function, including inhibiting secretion of granules, which mitigates cutaneous damage by sphingomyelinase D.[18] The use of either dapsone or surgical intervention however, for even moderate-to-severe necrosis, is controversial.[1]
The extensive dermonecrosis observed in our patient may be attributable to the tight-fitting football girdle garments worn for multiple hours following the bite. This compression could potentially have increased the amount of venom injected, limited dispersal of the venom by superficial lymphatic obstruction thus concentrating its effects, or impeded normal physiological/immunological responses that might mitigate the toxin’s damage. This case, therefore, highlights the potential ability of spider envenomation, likely by Cheiracanthium, to induce much more severe dermonecrosis than previously thought possible.
Acknowledgment
The authors would like to thank Dennis McNair, PhD, for his help in identifying the specimen aforementioned and Arthur Huen, MD, PhD, for his assistance in obtaining radiological images.
References
1. Sams HH, Dunnick CA, Smith ML, King LE. Necrotic arachnidism. J Am Acad Dermatol. 2001;44:561–573.
2. Anonymous. Necrotic arachnidism—Pacific Northwest, 1988–1996. MMWR Morb Mortal Wkly Rep. 1996;45:433–436.
3. Vetter RS, Isbister GK. Medical aspects of spider bites. Annu Rev Entomol. 2008;53:409–429.
4. Roe AH. The aggressive house spider (hobo spider). Utah State University 1993; Fact Sheet No.86:1–5.
5. Yan L, Adams ME. Lycotoxins, antimicrobial peptides from venom of the wolf spider Lycosa carolinensis. J Bio Chem. 1998;273(4):2059–2066.
6. Corzo G, Villegas E, Gomez-Lagunas F, et al. Oxyopinins, large amphipathic peptides isolated from the venom of the wolf spider Oxyopes kitabensis with cytolytic properties and positive insecticidal cooperativity with spider neurotoxins. J Biol Chem. 2002;277(26)23627–23637.
7. Meinwald J, Eisner T. The chemistry of phyletic dominance. Proc Nat Acad Sci. 1995;92(1):14–18.
8. Foradori MJ, Smith SC, Smith E, Wells RE. Survey for potentially necrotizing spider venoms, with special emphasis on Cheiracanthium mildei. Comp Biochem Physiol C Toxicol Pharmacol. 2005;141(1):32–39.
9. Krinsky WL. Envenomation by the sac spider Chiracanthium mildei. Cutis. 1987;40:127–129.
10. Owri M. Envenomation of Chiracanthium japonicum and the properties of the venom. Jpn J Med Sci Biol. 1978;31:200–203.
11. Vetter RS, Isbister GK, Bush SP, Boutin LJ. Verified bites by yellow sac spiders (genus Cheiracanthium) in the United States and Australia: where is the necrosis? Am J Trop Med Hyg. 2006;74:1043–1048.
12. Spielman A, Levi HW. Probable envenomation by Chiracanthium mildei; a spider found in houses. Am J Trop Med Hyg. 1970;19:729–732.
13. Newlands G, Martindale CB, Berson SD, Rippey JJ. Cutaneous necrosis caused by the bite of Chiracanthium spiders. S Afr Med J. 1980;57:171–173.
14. Maretic Z. Chiracanthium punctorium Villers—eine europaische Giftspinne. Med Klin. 1962;37:1576–1577.
15. Swanson DL, Vetter RS. Bites of brown recluse spiders and suspected necrotic arachnidism. N Engl J Med. 2005;352(7):700–707.
16. Swanson DL, Vetter RS. Loxoscelism. Clin Dermatol. 2006;24(3):213–221.
17. King LE, Rees RS. Dapsone treatment of brown recluse bite. JAMA. 1983;250:648.
18. Patel KD, Modur V, Zimmerman GA, et al. The necrotic venom of the brown recluse spider induces dysregulated endothelial cell-dependent neutrophil activation. J Clin Invest.1994;94:631–642.